
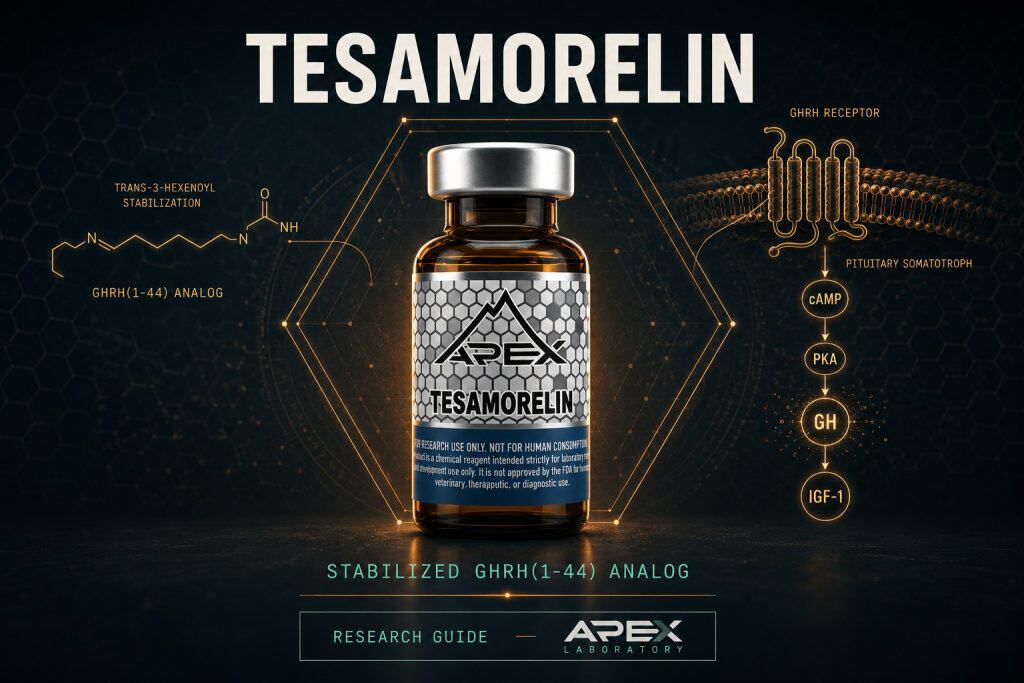
Tesamorelin is a synthetic, stabilized analog of human growth-hormone-releasing hormone, GHRH(1-44), carrying an N-terminal trans-3-hexenoyl group on Tyr1 that confers resistance to dipeptidyl peptidase-4 and slows plasma degradation. It engages the GHRH receptor, a Class B G-protein-coupled receptor on pituitary somatotrophs, driving cAMP-mediated pulsatile growth-hormone release and downstream hepatic IGF-1. Apex Laboratory supplies tesamorelin as a research-grade chemical reagent for in-vitro and preclinical research, distinct from the Egrifta pharmaceutical formulation.
Within the growth-hormone-releasing hormone (GHRH) analog family, tesamorelin sits a step removed from the foundational members. Where sermorelin reproduces only the minimal receptor-active GHRH(1-29) fragment and CJC-1295 extends duration through an albumin-binding Drug Affinity Complex, tesamorelin takes the opposite design route: it retains the complete 44-residue GHRH sequence and stabilizes the molecule chemically at its most vulnerable point. Originally developed by Theratechnologies under the research designation TH9507, it is built on the full hGRF(1-44)NH2 backbone and carries a single defining modification — an N-terminal trans-3-hexenoyl group on Tyr1 that resists the dipeptidyl peptidase-4 (DPP-4) cleavage that rapidly inactivates native GHRH.[1]
This guide profiles tesamorelin as a research-grade chemical reagent: its molecular identity, its GHRH-receptor mechanism, the chemistry behind its DPP-4 resistance, its pharmacokinetic behavior, the visceral-adipose research base that dominates its literature, and the structural reasons it differs from sermorelin. Throughout, the framing is research-context only — tesamorelin is studied here as a tool for growth-hormone-axis research, not characterized for any therapeutic use, and is categorically distinct from the FDA-approved Egrifta pharmaceutical formulation that shares the same molecule.
Tesamorelin at a Glance
- Tesamorelin is a synthetic, stabilized analog of human growth-hormone-releasing hormone built on the full-length GHRH(1-44) backbone, originally designated TH9507.
- Its defining structural feature is an N-terminal trans-3-hexenoyl ((E)-hex-3-enoyl) group on Tyr1 that confers resistance to dipeptidyl peptidase-4 (DPP-4) and slows plasma degradation.
- It acts as a GHRH-receptor agonist on a Class B G-protein-coupled receptor, engaging the Gαs/adenylyl-cyclase/cAMP/PKA cascade to stimulate endogenous pulsatile growth-hormone release.
- Unlike sermorelin, which corresponds to the shorter GHRH(1-29) fragment, tesamorelin combines the full GHRH(1-44) sequence with the trans-3-hexenoyl modification for greater enzymatic stability.
- The most-cited research base comes from the Falutz et al. phase 3 randomized controlled trials in HIV-associated lipodystrophy, reporting visceral-fat reduction and elevated IGF-I in trial populations.
- Apex supplies tesamorelin as a lyophilized research-grade reagent verified to ≥99% by HPLC and ESI-MS — categorically distinct from the FDA-approved Egrifta pharmaceutical formulation.
Tesamorelin
What Is Tesamorelin? Definition and Molecular Identity
Tesamorelin is a synthetic, stabilized analog of human growth-hormone-releasing hormone (GHRH), also historically called growth-hormone-releasing factor (GRF). Its peptide backbone reproduces the full-length 44-residue sequence, hGRF(1-44)NH2, with a C-terminal amide. The molecule is catalogued under CAS number 218949-48-5, with a molecular formula of C221H366N72O67S and a molecular weight of approximately 5135.9 g/mol; PubChem records the same composition under CID 16137828, where the IUPAC name explicitly begins with the (E)-hex-3-enoyl modification on the N-terminal tyrosine residue. The minor difference between the catalog mass of 5135.9 and the rounded PubChem value of roughly 5136 reflects rounding, not a discrepancy.
Reading the structure: backbone plus acyl cap
It helps to read the molecule in two parts. The first is the peptide chain itself: the complete 44-residue GHRH sequence, ending in a C-terminal amide (the NH2 in hGRF(1-44)NH2). The second is the single chemical addition that defines tesamorelin — the trans-3-hexenoyl group attached at the N-terminus. That two-part composition is why the molecule’s formula and mass are larger than the native peptide alone: the acyl modification adds atoms that show up in both the C221H366N72O67S formula and the roughly 5136 Da mass. For analytical work, this matters because mass-spectrometry identity confirmation targets that specific expected mass; a synthesis that omitted or altered the acyl cap would resolve to a different value.
The TH9507 research designation and the Egrifta connection
During its development by Theratechnologies, tesamorelin was identified as TH9507, the designation used across its early non-clinical and clinical literature.[1] The same molecule later became the active ingredient in the FDA-approved pharmaceutical formulation marketed as Egrifta. A research-grade reagent and that pharmaceutical formulation are the same chemical entity but occupy categorically distinct regulatory frameworks — a distinction examined in detail in a later section and in Apex’s research-grade versus pharmaceutical-grade peptides reference. For laboratory work, tesamorelin ships as a lyophilized powder; the molecular specifications above should always be confirmed against the lot-specific Certificate of Analysis rather than assumed from a catalog value. Researchers encountering the molecule under either the TH9507 designation or the Egrifta brand in the literature are reading about the same chemical entity described here.
GHRH-Analog Mechanism: GHRHR Class B GPCR Signaling
Tesamorelin works the same way the endogenous hormone it mimics does: by activating the GHRH receptor (GHRHR) on the somatotroph cells of the anterior pituitary. The GHRHR is a Class B (secretin-family) G-protein-coupled receptor. When an agonist occupies the receptor, it couples through the stimulatory G protein Gαs to adenylyl cyclase, raising intracellular cyclic AMP (cAMP); Cunha and Mayo at Northwestern University documented this canonical pathway, showing that GHRH-receptor activation drives adenylyl-cyclase activity and increased cAMP production in cells expressing the receptor.[2] The cAMP signal in turn activates protein kinase A (PKA), the proximate trigger for growth-hormone synthesis and pulsatile secretion. The released growth hormone then acts on peripheral tissues, most notably the liver, where it stimulates production of insulin-like growth factor 1 (IGF-1); the resulting GH and IGF-1 readouts are the downstream markers most often used to confirm axis engagement in the cited research.
GHRH receptor → Gαs → adenylyl cyclase → cAMP → PKA → pulsatile GH release → hepatic IGF-1
Tesamorelin binds the GHRH receptor (GHRHR), a Class B G-protein-coupled receptor on anterior-pituitary somatotrophs. Receptor occupancy couples through the stimulatory G protein Gαs to adenylyl cyclase, raising intracellular cyclic AMP; the cAMP signal then activates protein kinase A (PKA), the proximate driver of growth-hormone synthesis and pulsatile secretion. Cunha and Mayo documented this canonical GHRH-receptor-to-cAMP cascade in receptor-expressing cells.[2] Because the analog acts upstream at the receptor rather than supplying growth hormone directly, it preserves the episodic, pulsatile character of endogenous secretion and depends on a functioning somatotroph population.
Receptor biology beyond the canonical cascade
The receptor’s behavior is not limited to acute cAMP generation. Katsushima and colleagues characterized human GHRHR signal transduction and trafficking, reporting that the receptor’s C-terminus interacts with the scaffolding protein PICK1 to modulate cell-surface trafficking and downstream cAMP signaling — a layer of regulation relevant to how the receptor population responds over time.[3] Because tesamorelin acts upstream, at the receptor, rather than supplying growth hormone directly, its pharmacology depends on a functioning somatotroph population and preserves the episodic, pulsatile character of endogenous secretion. That mechanistic distinction — agonist at the GHRH receptor rather than exogenous hormone — is shared across the GHRH-analog family.
The Trans-3-Hexenoyl Modification: How Stabilization Works
The single feature that sets tesamorelin apart from unmodified GHRH is a small acyl group added to the front of the molecule. Native GHRH is rapidly inactivated in plasma, largely through cleavage near its N-terminus by dipeptidyl peptidase-4 (DPP-4), an enzyme that trims dipeptides from the amino-terminal end of susceptible peptides. Removing or blocking that vulnerable site is the central design problem for any long-lived GHRH analog.
Trans-3-hexenoyl addition to Tyr1
Tesamorelin solves it by attaching a trans-3-hexenoyl ((E)-hex-3-enoyl) moiety to Tyr1, the N-terminal tyrosine of the hGRF(1-44)NH2 backbone. Ferdinandi and colleagues, in the primary non-clinical pharmacology and safety evaluation of TH9507 published in Basic & Clinical Pharmacology & Toxicology, reported that this modification confers resistance to dipeptidyl aminopeptidase-IV (DPP-4) and slows the peptide’s degradation in rat, dog, and human plasma, prolonging its elimination kinetics while preserving the molecule’s ability to raise growth hormone and IGF-1 in their models.[1] In other words, the acyl cap shields the cleavage site without abolishing receptor engagement.
Why the chemistry matters for the research base
This stabilization is the mechanistic foundation for tesamorelin’s longer duration of action relative to unmodified GHRH, and it is the property that most clearly differentiates the molecule from the unmodified fragment used in sermorelin. It is worth stating plainly that DPP-4 resistance describes how the molecule behaves in the cited plasma and animal models; it is a pharmacologic characterization, not a claim about outcomes in any other context.
How Tesamorelin Differs From Sermorelin
Tesamorelin and sermorelin are often discussed together because both are GHRH-receptor agonists that engage the same Class B GPCR through the same Gαs/cAMP/PKA signaling. The differences are structural and pharmacokinetic rather than mechanistic at the receptor.
Fragment versus stabilized full-length
Sermorelin corresponds to GHRH(1-29) — the minimal N-terminal fragment that retains receptor activity. Tesamorelin retains the complete GHRH(1-44) sequence and adds the trans-3-hexenoyl group described above. The practical consequence reported in the literature is enzymatic stability: the modification that confers DPP-4 resistance is present on tesamorelin and absent from native sermorelin, which is the principal pharmacologic distinction between the two.[1]
Implications for duration of receptor engagement
Greater resistance to plasma degradation generally translates to a longer window of receptor engagement in research models, though the magnitude depends on species, assay, and study design. It is also worth noting that both compounds remain agonists at the same receptor with the same downstream signaling; the modification changes how long the molecule survives in plasma, not which receptor it activates or how. That is why direct head-to-head framing should focus on stability and duration rather than implying a different mechanism of action. Researchers comparing the two compounds directly should consult the dedicated tesamorelin versus sermorelin comparison and the broader sermorelin versus CJC-1295 analysis, both of which place the half-life and structural differences side by side. Comparative statements here should be read as research observations, not equivalence or superiority claims; each compound’s behavior is defined by its own cited literature.
Pharmacokinetics and Half-Life
Tesamorelin’s pharmacokinetics reflect its mechanism: rather than maintaining a sustained elevation, it produces a finite, episodic stimulus to growth-hormone secretion. Gonzalez-Sales and colleagues built a population pharmacokinetic/pharmacodynamic model from a phase I dataset (subjects receiving 1 or 2 mg subcutaneously daily for 14 days) and described tesamorelin as stimulating growth-hormone secretion in an episodic, finite-duration manner that then drives IGF-1 — a sequential PK/PD relationship rather than a single sustained plateau.[4]
Reading the half-life figures carefully
Half-life values for tesamorelin must be cited with their context. The frequently quoted apparent elimination half-life of roughly 21 to 45 minutes comes from the preclinical work of Ferdinandi and colleagues and was measured in dogs, not humans.[1] It should not be presented as a human value. The more appropriate human-relevant characterization is the population PK/PD description of episodic, finite-duration GH stimulation, which captures the pulsatile pharmacology better than any single clean human half-life number.[4] In the cited research protocols the compound is administered subcutaneously; reconstitution and handling for in-vitro work follow standard peptide practice described in the Apex peptide reconstitution guide.
Visceral Adipose Tissue: The Lipodystrophy Research Base
The largest and most-cited body of tesamorelin research comes from a series of phase 3 randomized controlled trials in HIV-associated lipodystrophy, conducted largely by Falutz and colleagues at the Montreal General Hospital and McGill University Health Centre, with collaborators including the Grinspoon group. These trials are summarized here strictly as research observations in their specific study population.
The Falutz pivotal trials
In the pivotal trial published in the New England Journal of Medicine in 2007, 412 patients received daily subcutaneous tesamorelin or placebo for 26 weeks; the tesamorelin group showed a 15.2% reduction in visceral adipose tissue compared with a 5.0% increase under placebo, alongside an 81.0% rise in IGF-I and improvements in triglycerides and the total-to-HDL cholesterol ratio.[5] A second phase 3 trial with a safety extension, also led by Falutz, confirmed the visceral-fat reduction and reported that the benefit reversed when participants were switched from tesamorelin to placebo.[6] A pooled analysis of the two pivotal trials (806 participants) reported a visceral-adipose-tissue treatment effect of roughly -15.4% at week 26, maintained at about -17.5% at week 52.[7]
Durability and reversibility
Long-term safety and effect data over 52 weeks, again from the Falutz group, reported that the visceral-fat reduction was sustained over the year and that visceral fat reaccumulated on discontinuation — consistent with a mechanism that depends on ongoing receptor engagement rather than a permanent structural change.[8] Stanley and colleagues in the Grinspoon group further linked the magnitude of visceral-fat reduction to an improved metabolic profile, reporting that responders with at least an 8% reduction had significantly improved triglycerides and adiponectin and preserved glucose homeostasis over 52 weeks.[9] These findings define the visceral-fat research base; they are trial observations in a defined clinical population, not statements about research-grade reagent use.
Hepatic Fat and NAFLD Research Findings
Beyond visceral adipose tissue, a distinct strand of research has examined tesamorelin and liver fat, an endpoint that is related to but separate from visceral fat. This work also originates largely from the Grinspoon group at Massachusetts General Hospital and Harvard.
Tesamorelin and non-alcoholic fatty liver disease
Stanley and colleagues reported a randomized, double-blind, multicentre trial of tesamorelin in HIV-associated non-alcoholic fatty liver disease (NAFLD), published in The Lancet HIV in 2019, in which 12 months of daily tesamorelin was associated with a reduction in hepatic fat fraction relative to placebo.[10] Fourman and colleagues separately connected the two endpoints, reporting that among patients with elevated baseline liver enzymes, those who responded to tesamorelin with visceral-fat reduction also showed greater reductions in ALT and AST over the trial period.[11]
Why the endpoints are kept distinct
Hepatic-fat and visceral-fat measures track related but non-identical compartments, and the research literature reports them separately. Keeping the two endpoints distinct matters for accurate interpretation: a visceral-fat result does not automatically imply a hepatic-fat result, and the citations above measure each directly. As with the visceral-fat data, these are trial findings in a specific clinical population summarized for research context only.
Beyond Lipodystrophy: GH/IGF-1 Axis in Other Research Populations
A smaller set of studies has examined GHRH-analog pharmacology outside the HIV-lipodystrophy setting. These are included here only to illustrate how the GHRH/GH/IGF-1 axis engages across research populations — they are not approved or established uses, and they should not be read as therapeutic extrapolation.
Non-HIV obese subjects with reduced GH secretion
Makimura and colleagues at Massachusetts General Hospital conducted a randomized controlled trial of the growth-hormone-releasing factor analog in non-HIV obese subjects with reduced growth-hormone secretion, reporting a selective reduction in visceral adipose tissue with an increase in IGF-I and no aggravation of glucose homeostasis in that population.[12] This indicates the visceral-adipose and IGF-1 responses are not unique to HIV-associated lipodystrophy.
GHRH and cognitive-function research
Baker and colleagues at the University of Washington studied tesamorelin — described in their report as a stabilized analog of human GHRH — administered subcutaneously for 20 weeks in adults with mild cognitive impairment and healthy older adults, reporting axis engagement with an increase in IGF-1 within the physiological range.[13] The cognitive endpoint in that trial is investigational and is referenced here only as evidence of GHRH/GH/IGF-1 axis engagement in a non-lipodystrophy population — not as any characterization of cognitive benefit.
Comparator Pharmacology: GHRH-Analog Family
Placing tesamorelin against its closest relatives clarifies where its design choices sit. Sermorelin, tesamorelin, and CJC-1295 are all GHRH-receptor agonists targeting the same Class B GPCR through Gαs/cAMP/PKA signaling; they differ chiefly in structure, stabilization strategy, plasma half-life, and regulatory status. The table below summarizes those differences for research orientation; the per-compound half-life and status figures should always be confirmed against each compound’s own cited literature.
Tesamorelin vs Sermorelin vs CJC-1295 with DAC
| Property | Tesamorelin | Sermorelin | CJC-1295 with DAC |
|---|---|---|---|
| Backbone | Stabilized GHRH(1-44) full length | GHRH(1-29) N-terminal fragment | Modified GHRH(1-29) + DAC linker |
| Stabilization | N-terminal trans-3-hexenoyl on Tyr1 (DPP-4 resistance) | None (native sequence) | Albumin-binding Drug Affinity Complex (DAC) |
| Plasma half-life | ~26-38 min | ~10-20 min | ~8 days |
| Receptor / signaling | GHRHR agonist (Gαs/cAMP/PKA) | GHRHR agonist (Gαs/cAMP/PKA) | GHRHR agonist (Gαs/cAMP/PKA) |
| FDA status | Approved as Egrifta® (app 022505, Nov 10, 2010; HIV lipodystrophy) | Historical Geref® (approved 1990 + 1997; withdrawn 2008) | No FDA approval (clinical investigation) |
| Apex availability | Research-grade ≥99% lyophilized | Research-grade ≥99% lyophilized | Research-grade ≥99% lyophilized |
Two points deserve emphasis. First, tesamorelin and sermorelin pursue opposite structural strategies — full-length-plus-acyl-cap versus minimal fragment — while CJC-1295 with DAC pursues a third route entirely, using an albumin-binding Drug Affinity Complex to extend half-life into the multi-day range, as detailed in the CJC-1295 research guide. Second, regulatory status diverges sharply across the family: tesamorelin’s molecule is FDA-approved as a pharmaceutical formulation, sermorelin’s was historically approved and later commercially withdrawn, and the CJC-1295 variants remain in investigation. Those distinctions are explored further in the dedicated tesamorelin versus sermorelin comparison.
Synthesizing the Evidence: Meta-Analytic Perspective
A recent meta-analysis allows the scattered trial data to be viewed in aggregate while keeping its limits in view. Badran and colleagues, publishing in Obesity Research & Clinical Practice in 2026, pooled randomized controlled trials of tesamorelin in HIV-associated lipodystrophy and reported significant reductions in visceral adipose tissue, trunk fat, hepatic fat percentage, and waist circumference, together with an increase in lean mass; the most commonly reported adverse events across trials were arthralgia, myalgia, paresthesia, and injection-site reactions.[14]
Consistency, heterogeneity, and what remains uncertain
The aggregate picture is internally consistent with the individual Falutz and Grinspoon-group trials, which is reassuring for the body-composition signal. Several caveats temper interpretation, however. The research base is concentrated in a single clinical population (HIV-associated lipodystrophy) and a small number of research networks, which limits generalizability. Half-life figures are heterogeneous and partly preclinical, as discussed above. And a meta-analysis is a secondary synthesis: the load-bearing numbers still come from the primary randomized trials. Effect-size language should therefore stay measured — the data describe consistent visceral- and hepatic-fat reductions within studied populations, not established outcomes in any other setting.
Research-Grade Tesamorelin vs Egrifta: Distinct Regulatory Frameworks
Tesamorelin is one of the clearest examples of a molecule that exists simultaneously as an FDA-approved pharmaceutical product and as a research-grade chemical reagent. Same molecule (tesamorelin); categorically distinct regulatory frameworks. Understanding that distinction is essential for accurate research-context framing.
Egrifta: FDA approval and regulatory facts
The pharmaceutical formulation of tesamorelin is marketed as Egrifta (with later formulations Egrifta SV and Egrifta WR). It holds FDA application number 022505 and was originally approved on November 10, 2010, with Theratechnologies Inc. of Montreal, Canada as the sponsor. Its approved indication is the reduction of excess abdominal fat in HIV-infected adult patients with lipodystrophy; the labeling notes that it is not indicated for weight-loss management and that long-term cardiovascular safety has not been established. (Historical US co-marketing arrangements for the brand are sometimes cited in secondary sources; this guide attributes the molecule’s development and sponsorship to Theratechnologies, which is the verified record.)
Why a research-grade reagent is not a pharmaceutical
A research-grade reagent shares Egrifta’s chemical identity but is a lyophilized chemical supplied for in-vitro and preclinical research only. It is not a pharmaceutical, not for human consumption, and not therapeutically equivalent to the approved formulation. This is the same regulatory logic Apex applies across same-molecule compounds, set out in the research-grade versus pharmaceutical-grade peptides reference. The existence of an approved drug product does not convert a research reagent into a therapeutic, and nothing in this guide should be read as promoting research-grade tesamorelin as equivalent to Egrifta.
COA, HPLC and ESI-MS: The Purity Trust Angle
For peptide research to be reproducible, the identity and purity of the reagent must be documented, not assumed. Tesamorelin’s relatively large molecular weight (around 5136 Da) and its acyl modification make analytical verification particularly important — small synthesis differences can change behavior in sensitive assays.
HPLC purity and ESI-MS identity confirmation
Apex research-grade tesamorelin is supplied at a target of ≥99% purity verified by reversed-phase high-performance liquid chromatography (HPLC), with molecular identity confirmed by electrospray-ionization mass spectrometry (ESI-MS) against the expected mass of roughly 5136 Da. Each lot is accompanied by a per-batch Certificate of Analysis, archived in the Apex lab-verified COA archive. Researchers can review the methodology behind these checks in the Apex references on HPLC purity testing, mass-spectrometry verification, and how to read a peptide COA. The stated purity threshold is lot-specific and documented on the COA rather than guaranteed in the abstract.
Storage and handling of lyophilized tesamorelin
The lyophilized powder is stored at -20°C, protected from light and moisture; reconstituted solution is kept cold and used per protocol, following the general handling discipline described in the Apex peptide storage guide and reconstitution guide. As with all research reagents, aliquoting before refrigerated storage and minimizing freeze-thaw cycles help preserve integrity for longer-duration in-vitro work.
Why verification underpins reproducibility
The reason these checks are non-negotiable for serious peptide research is reproducibility: an assay result is only as trustworthy as the identity and purity of the material that produced it. A reagent that is mislabeled, under-purity, or chemically altered can generate data that cannot be replicated, wasting experimental effort and confounding comparisons across studies. Documenting purity by HPLC and identity by ESI-MS on a per-lot basis — rather than relying on a generic catalog claim — is what allows a researcher to attribute an observed effect to the intended molecule. For tesamorelin specifically, confirming both the expected mass and the presence of the trans-3-hexenoyl modification is the analytical signature that distinguishes it from the unmodified GHRH fragment and from degraded material.
Safety, Tolerability & Adverse-Event Observations (Research Context)
The tesamorelin literature includes a substantial tolerability record, because the pivotal program in HIV-associated lipodystrophy carried dedicated safety extensions. These are documented findings in defined clinical-trial populations, reported here strictly as research observations — they are not patient guidance, not a description of what any individual should expect, and not characterizations of research-grade reagent use.
Adverse events reported across the controlled trials
In the published clinical research, the most frequently reported adverse events were generally mild musculoskeletal and local effects. The 2026 meta-analysis by Badran and colleagues, pooling randomized controlled trials in HIV-associated lipodystrophy, reported arthralgia, myalgia, paresthesia, and injection-site reactions as the most commonly observed adverse events across the trial set.[14] The two pivotal phase 3 trials and their pooled analysis, led by Falutz and colleagues, similarly described the compound as generally well tolerated over the controlled treatment periods, with the safety-extension design specifically built to capture longer-exposure observations.[6][7]
Glucose homeostasis and longer-exposure findings
Because the compound raises IGF-1, glucose handling was a pre-specified safety concern in these trials. The 52-week long-term safety report from the Falutz group described sustained visceral-fat reduction without aggravation of glucose homeostasis over the year of observation.[8] The non-HIV trial by Makimura and colleagues likewise reported no aggravation of glucose homeostasis in obese subjects with reduced growth-hormone secretion.[12] It is worth stating plainly that the FDA labeling for the corresponding pharmaceutical formulation notes that long-term cardiovascular safety has not been established — a regulatory limitation, not a research-reagent property, and one more reason these data describe a specific clinical context rather than research-grade reagent handling.
How dosing appeared in the published studies
For research-context orientation only, it is useful to note the doses these tolerability observations are attached to. The cited trials administered tesamorelin by subcutaneous injection, most commonly at 2 mg daily in the pivotal lipodystrophy program, with the phase I pharmacokinetic work of Gonzalez-Sales and colleagues using 1 or 2 mg daily for 14 days.[4] These are reported here as study facts describing how the published research was conducted — not as a recommended dose, protocol, or any guidance for use. Apex supplies tesamorelin solely as a lyophilized reagent for in-vitro and preclinical research, and any laboratory handling follows the general discipline described in the Apex peptide reconstitution guide and peptide storage guide rather than any clinical regimen.
Sourcing Research-Grade Tesamorelin
Apex Laboratory supplies tesamorelin as a lyophilized, research-grade chemical reagent for in-vitro and preclinical research only. Each lot is verified to a target of ≥99% purity by HPLC, with identity confirmed by electrospray-ionization mass spectrometry (ESI-MS), and ships with a per-batch Certificate of Analysis available through the lab-verified COA archive. The methodology and editorial sourcing standards behind every product are documented in the Apex editorial standards, and adjacent GHRH-analog reagents — including the foundational sermorelin fragment and the long-acting CJC-1295 with DAC — allow researchers to assemble a comparison panel across the family. None of these reagents is a pharmaceutical or intended for human consumption.
tesamorelin and Adjacent Research Reagents
Tesamorelin
Stabilized GHRH(1-44) analog research reagent with N-terminal trans-3-hexenoyl modification; supplied at ≥99% purity verified by HPLC and mass spectrometry.
View ProductSermorelin Acetate
GHRH(1-29) N-terminal fragment; the foundational unmodified GHRH-analog comparator.
View ProductCJC-1295 with DAC
Long-acting GHRH analog with a Drug Affinity Complex albumin-binding linker for extended half-life research.
View ProductFrequently Asked Questions
What is tesamorelin and how does it work?
Tesamorelin is a synthetic, stabilized analog of human growth-hormone-releasing hormone, GHRH(1-44), carrying a trans-3-hexenoyl modification on its N-terminal tyrosine. In the published research it binds the GHRH receptor, a Class B G-protein-coupled receptor on pituitary somatotrophs, activating the Gαs/adenylyl-cyclase/cAMP pathway to stimulate endogenous, pulsatile growth-hormone release and subsequent hepatic IGF-1 production. It is studied as a research reagent and is not characterized here for any therapeutic use.
How is tesamorelin different from sermorelin?
Both are GHRH-receptor agonists, but they differ in structure and stability. Sermorelin corresponds to the GHRH(1-29) fragment, whereas tesamorelin is built on the full-length GHRH(1-44) sequence with an added trans-3-hexenoyl group. Ferdinandi and colleagues reported that this modification confers resistance to dipeptidyl peptidase-4 (DPP-4) and slows plasma degradation, which is the principal pharmacologic distinction described in the literature. Comparative claims should be read as research observations, not equivalence statements.
Is research-grade tesamorelin the same as Egrifta?
They share the same molecule but occupy categorically distinct regulatory frameworks. Egrifta and Egrifta SV are FDA-approved pharmaceutical formulations of tesamorelin (FDA application 022505, originally approved November 10, 2010, Theratechnologies) indicated for reducing excess abdominal fat in HIV-infected adults with lipodystrophy. A research-grade reagent is a lyophilized chemical supplied for in-vitro and preclinical research only; it is not a pharmaceutical, not for human consumption, and not therapeutically equivalent.
What is the half-life of tesamorelin?
Tesamorelin has a short circulating half-life and acts in an episodic fashion, producing a finite-duration pulse of growth hormone rather than sustained elevation, as described in population pharmacokinetic/pharmacodynamic modeling by Gonzalez-Sales and colleagues. Preclinical work by Ferdinandi et al. reported an apparent elimination half-life of roughly 21-45 minutes in dogs; species and assay differences mean exact human values should be drawn from the specific study being cited rather than generalized.
What doses of tesamorelin were used in published studies?
Reported as study facts only, not as guidance: the pivotal phase 3 trials in HIV-associated lipodystrophy administered tesamorelin by subcutaneous injection at 2 mg daily, and the phase I pharmacokinetic work used 1 or 2 mg daily for 14 days. These figures describe how the published research was conducted in defined clinical populations. They are not a recommended dose or protocol, and Apex supplies tesamorelin only as a research reagent for in-vitro and preclinical work.
What adverse events have been reported in tesamorelin clinical trials?
In the published clinical research, the most commonly reported adverse events were generally mild. A 2026 meta-analysis of randomized controlled trials in HIV-associated lipodystrophy reported arthralgia, myalgia, paresthesia, and injection-site reactions most frequently. Long-term Falutz-group data described the compound as generally well tolerated without aggravation of glucose homeostasis over 52 weeks. These are trial observations in specific study populations summarized for research context, not patient guidance or descriptions of reagent use.
How is research-grade tesamorelin reconstituted and stored?
Use the peptide reconstitution calculator to convert vial mass and bacteriostatic-water volume into concentration and syringe-unit values for research preparations.
As a general research-handling matter, lyophilized tesamorelin is typically stored at -20 degrees C, protected from light and moisture, and reconstituted with an appropriate sterile diluent following standard peptide practice; reconstituted solution is kept cold, aliquoted, and protected from repeated freeze-thaw to preserve integrity. Apex documents this discipline in its peptide reconstitution guide and peptide storage guide. These notes describe in-vitro laboratory handling, not any clinical preparation or administration.
Why does the trans-3-hexenoyl modification matter?
Native GHRH is rapidly inactivated in plasma, largely by dipeptidyl peptidase-4 (DPP-4) cleavage near its N-terminus. Adding a trans-3-hexenoyl ((E)-hex-3-enoyl) group to the N-terminal tyrosine of GHRH(1-44), as reported by Ferdinandi et al., slows that degradation and prolongs the peptide’s plasma elimination kinetics. In the literature this stabilization is the basis for tesamorelin’s extended duration of action relative to unmodified GHRH.
Continue Your Research
Researchers building broader context across the Apex Research Library may find the following references useful:
- Growth Hormone Axis Research Peptides — The cluster hub situating tesamorelin among GHRH analogs and secretagogues.
- Tesamorelin vs Sermorelin — Direct structural and pharmacokinetic comparison of the two GHRH analogs.
- Sermorelin Research Guide — The foundational GHRH(1-29) fragment and unmodified comparator.
- CJC-1295 Research Guide — The long-acting DAC-linked GHRH analog with a multi-day half-life.
- Sermorelin vs CJC-1295 — Lateral comparison covering half-life and stabilization-strategy contrasts.
- Research-Grade vs Pharmaceutical-Grade Peptides — The same-molecule, distinct-framework logic behind tesamorelin and Egrifta.
- How to Read a Peptide COA — Interpreting HPLC purity and ESI-MS identity data on a Certificate of Analysis.
- Peptide Storage Guide — Handling lyophilized and reconstituted peptides to preserve integrity.
Research Use Disclaimer
This guide is provided for research and educational purposes only. Tesamorelin supplied by Apex Laboratory is a research-grade chemical reagent intended exclusively for in-vitro and preclinical laboratory research. It is not a drug, not a dietary supplement, and not for human or veterinary consumption, diagnosis, treatment, or any clinical use. Although tesamorelin shares its molecular identity with the FDA-approved pharmaceutical formulation marketed as Egrifta, the research-grade reagent occupies a categorically distinct regulatory framework and is not therapeutically equivalent to, nor a substitute for, that approved formulation — see research-grade versus pharmaceutical-grade peptides. All clinical-trial findings referenced here are summarized as research observations in their original study populations and do not constitute therapeutic or efficacy claims. Researchers are responsible for compliance with all applicable laws, institutional policies, and safe-handling requirements.
