
Tesamorelin and Sermorelin occupy a distinctive position among GHRH analogs in research circulation: both have passed FDA registrational review, at different points in pharmaceutical history, under different sponsors, for different indications. Tesamorelin is the active ingredient in Egrifta® (FDA-approved November 10, 2010 under NDA 22-505 for HIV-associated lipodystrophy in adults; sponsor Theratechnologies). Sermorelin acetate is the active ingredient in Geref®, which was FDA-approved on September 26, 1997 under NDA 20-443 for pediatric idiopathic growth hormone deficiency, building on an earlier December 1990 diagnostic approval under NDA 19-863, before being voluntarily withdrawn from the US market in 2008 for commercial reasons — not safety. No other comparison in the Apex catalog pairs two compounds with this dual-registrational pedigree, making the side-by-side study one of the more instructive in GH-axis research.
This guide provides a detailed, evidence-based, side-by-side comparison of Tesamorelin and Sermorelin for researchers — covering structural lineage from native GHRH(1-44), receptor pharmacology at GHRH-R, registrational research history under separate FDA NDAs, key published clinical literature, and Apex Laboratory’s research-grade catalog availability. Throughout, the comparison is framed around research-design questions rather than therapeutic preference: neither compound is “better”; they sit at different points in the GHRH-analog structural lineage and at different points in the regulatory-status spectrum.
Tesamorelin vs Sermorelin at a Glance
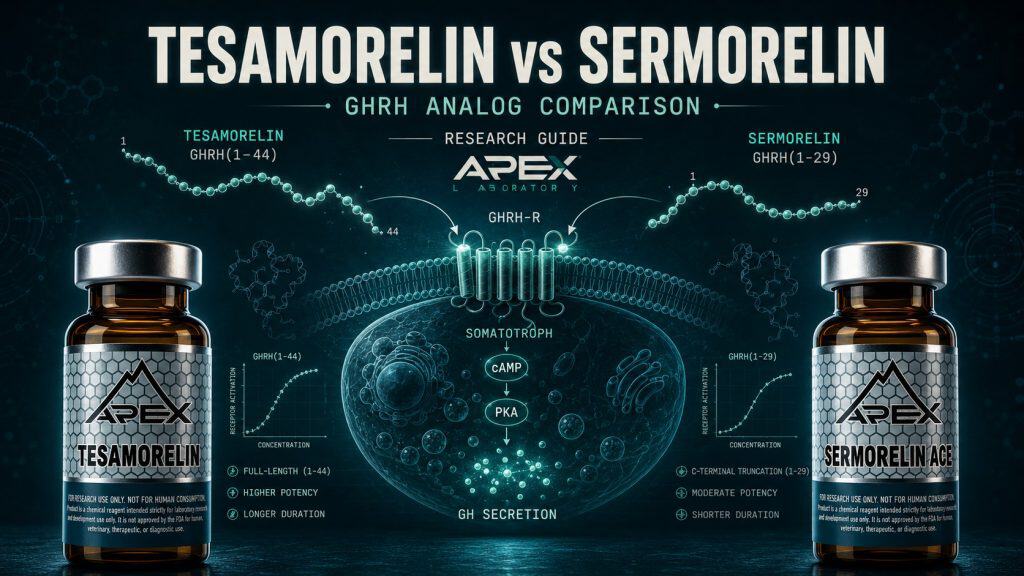
- Tesamorelin is a stabilized full-length GHRH(1-44) analog with an N-terminal trans-3-hexenoyl modification; Sermorelin is the GHRH(1-29)NH2 synthetic 29-residue N-terminal fragment of native GHRH — same receptor (GHRH-R), different structural strategies for solving the same plasma-stability problem
- Tesamorelin is the active ingredient in Egrifta® (FDA-approved November 10, 2010 under NDA 22-505 for HIV-associated lipodystrophy in adults; Egrifta SV® reformulation 2019); Sermorelin was the active ingredient in Geref® (FDA-approved September 26, 1997 under NDA 20-443 for pediatric GHD with earlier December 1990 diagnostic NDA 19-863; voluntarily withdrawn from the US market 2008 for commercial reasons, not safety)
- Plasma half-life diverges with structural strategy: Tesamorelin approximately 26-38 minutes (DPP-IV-blocked N-terminus), Sermorelin approximately 11-12 minutes (unmodified Tyr-Ala N-terminus susceptible to DPP-IV cleavage as characterized by Frohman 1989); both support once-daily subcutaneous research-context administration
- Tesamorelin’s clinical evidence base is the Egrifta® Phase 3 registrational program (Falutz 2007 NEJM, Falutz 2010 JCEM pooled, Falutz 2010 JAIDS, plus Stanley and Mangili post-registration extensions); Sermorelin’s clinical evidence base is the Geref® pediatric GHD registrational program (Thorner 1996 JCEM Geref International Study Group) plus older-adult GH-axis restoration literature (Khorram 1997, Walker 2006)
- Apex Laboratory’s research-grade Tesamorelin and Sermorelin Acetate are chemical research reagents distinct from the approved Egrifta® / Egrifta SV® and previously-approved Geref® pharmaceutical formulations — both supplied at ≥99% purity verified by HPLC and mass spectrometry for in-vitro and preclinical research only
The Two GHRH Analogs at a Glance
Tesamorelin and Sermorelin share the same molecular target — the pituitary growth hormone-releasing hormone receptor (GHRH-R) — but diverge sharply on structural class, sequence length, pharmacokinetic stability, and current regulatory status. Both are research-grade chemical reagents in the Apex Laboratory catalog. The 9-row comparison table below summarizes the load-bearing distinctions; the article’s H2 sections then unpack each row in turn. A third structurally-related compound, CJC-1295 with DAC, sits adjacent to both as a longer-acting GHRH(1-29) analog with an albumin-binding maleimide modification — characterized by Teichman and colleagues13 in 2006 — and is included in the Apex catalog grid below as a third-compound bridge for researchers building broader GHRH-analog context. Researchers comparing the two main subjects of this guide should focus on three axes: structural lineage (full-length stabilized GHRH(1-44) versus GHRH(1-29)NH2 N-terminal fragment), regulatory trajectory (currently-approved Egrifta® versus previously-approved Geref® withdrawn 2008 for commercial reasons), and the pharmacokinetic consequence of the structural differences.
Tesamorelin vs Sermorelin
| Attribute | Tesamorelin | Sermorelin |
|---|---|---|
| Origin / discovery program | Theratechnologies stabilized GHRH analog program; built on the 44-residue native GHRH characterized by Guillemin and Rivier groups in 1982 | Synthetic 29-residue N-terminal fragment of native GHRH; clinical pharmacology developed by Vance, Thorner, Vale, and Rivier groups from 1986 |
| Structural class | Stabilized full-length GHRH(1-44) analog with N-terminal trans-3-hexenoyl modification | GHRH(1-29)NH2 N-terminal fragment; C-terminal Arg29 capped as primary amide; no N-terminal modification |
| Sequence length (residues) | 44 amino acids plus N-terminal trans-3-hexenoyl group | 29 amino acids |
| Half-life | Approximately 26–38 minutes plasma half-life (DPP-IV blocked) | Approximately 11–12 minutes plasma half-life (DPP-IV-susceptible Tyr-Ala N-terminus) |
| Administration route | Daily subcutaneous injection (Egrifta® 2 mg/day Phase 3 dose; Egrifta SV® 2019 reformulation streamlined reconstitution) | Daily subcutaneous injection (Geref® therapeutic 0.5 / 1.0 mg/vial) |
| Receptor target | GHRH receptor (GHRH-R) on pituitary somatotrophs (Mayo 1992 cloning) | GHRH receptor (GHRH-R) on pituitary somatotrophs — same target as Tesamorelin |
| Regulatory status | Active ingredient in Egrifta® (FDA-approved November 10, 2010 under NDA 22-505 for HIV-associated lipodystrophy in adults; Egrifta SV® reformulation 2019); sponsor Theratechnologies | Was the active ingredient in Geref® (FDA-approved September 26, 1997 under NDA 20-443 for pediatric GHD; earlier December 1990 diagnostic NDA 19-863); voluntarily withdrawn from US market 2008 for commercial reasons, not safety |
| Apex catalog availability | Available as research-grade chemical reagent at ≥99% purity; distinct from approved Egrifta® / Egrifta SV® pharmaceutical formulations | Available as research-grade Sermorelin Acetate at ≥99% purity; distinct from previously-approved Geref® formulations |
| Research-context use cases | Stabilized-analog pharmacology, DPP-IV-resistance SAR, HIV-associated lipodystrophy mechanism, post-registration metabolic-endpoint extension studies | GHRH(1-29) fragment pharmacology, pediatric GHD registrational research lineage, older-adult GH-axis restoration paradigms |
Structural Lineage: Full-Length GHRH(1-44) vs N-Terminal Fragment GHRH(1-29)NH2
The structural relationship between Tesamorelin and Sermorelin starts with native human growth hormone-releasing hormone (GHRH) — the 44-residue hypothalamic peptide first characterized in 1982 by two independent groups working on human pancreatic islet tumors that caused acromegaly. Guillemin and colleagues at the Salk Institute1 reported the structure in Science; Rivier, Spiess, Thorner, and Vale2 reported the parallel characterization in Nature. Both papers established the 44-residue length and the GH-releasing activity from which every GHRH analog in research circulation traces.
Tesamorelin: Stabilized Full-Length GHRH(1-44)
Tesamorelin retains the full 44-residue length of native GHRH and adds a single N-terminal modification — a trans-3-hexenoyl group attached to the amino-terminus. This modification was engineered to block proteolytic cleavage by dipeptidyl peptidase IV (DPP-IV), the plasma enzyme that rapidly degrades native GHRH. Frohman and colleagues4 demonstrated in 1989 that DPP-IV cleaves human GHRH at the N-terminal Tyr-Ala bond, producing the inactive GHRH(3-44) fragment with a circulating half-life of only minutes. Tesamorelin’s N-terminal cap blocks DPP-IV access to that bond, extending plasma half-life into the ~26–38 minute range that supports once-daily subcutaneous dosing in the registrational program.
Sermorelin: GHRH(1-29)NH2 N-Terminal Fragment
Sermorelin is the synthetic 29-residue N-terminal fragment of native GHRH — the first 29 amino acids of the parent 44-residue peptide, with the C-terminal Arg29 capped as primary amide (-NH2). This fragment-based design rests on a finding from the original GHRH characterization work: GHRH-R binding affinity is concentrated in the N-terminal residues, so a 29-residue truncation retains receptor activation while simplifying synthesis. Sermorelin carries no N-terminal modification, so DPP-IV access to the Tyr-Ala bond is preserved — yielding a plasma half-life of approximately 11–12 minutes. CJC-1295 with DAC, by contrast, is also a GHRH(1-29) analog but adds a maleimide drug-affinity-complex (DAC) for covalent albumin binding, extending half-life to multi-day ranges13 — the same fragment scaffold as Sermorelin with an entirely different stabilization strategy.
Why the Structural Distinction Matters
The full-length-versus-fragment distinction is not just a length difference. It reflects two different engineering strategies for solving the same problem (GHRH’s short half-life): retain the parent length and block proteolysis at the N-terminus (Tesamorelin), or truncate to the binding-essential N-terminus and accept the shorter half-life (Sermorelin). Both yield active GHRH-R agonists. Researchers studying GH-axis pulsatility, GHRH-R pharmacology, or stabilized-analog structure-activity relationships choose between them based on which structural axis matters for the experimental question.
Tesamorelin: Stabilized Full-Length Analog and Egrifta® Registrational Program
Tesamorelin is the active ingredient in Egrifta® (FDA-approved November 10, 2010 under NDA 22-505 for HIV-associated lipodystrophy in adults; sponsor Theratechnologies). A reformulated single-vial version, Egrifta SV®, received FDA approval in 2019. Apex Laboratory’s research-grade Tesamorelin is classified as a chemical research reagent and is distinct from the approved Egrifta® / Egrifta SV® formulations.
Phase 3 Registrational Program
The Egrifta® approval rests on two pivotal Phase 3 randomized placebo-controlled trials in HIV-infected patients with abdominal-fat accumulation. The first, published in the New England Journal of Medicine by Falutz and colleagues5 in 2007, randomized 412 patients to tesamorelin 2 mg daily subcutaneous or placebo over 26 weeks. Visceral adipose tissue decreased 15.2% in the tesamorelin arm versus a 5.0% increase in the placebo arm. The second pivotal trial, published in the Journal of Acquired Immune Deficiency Syndromes by Falutz and colleagues17 in 2010, replicated the visceral-fat-reduction signal in a second multicenter trial with a safety extension. Falutz and colleagues6 then pooled both trials in a 2010 Journal of Clinical Endocrinology and Metabolism analysis with a 52-week safety extension, documenting sustained visceral-fat reduction with acceptable tolerability. These three publications together formed the registrational evidence package supporting Egrifta® FDA approval.
Long-Term Safety and Mechanistic Extensions
Beyond the headline efficacy endpoints, Falutz and colleagues7 published a 2008 AIDS open-label extension trial documenting tolerability beyond the registrational 26-week window. Stanley and colleagues15 extended the mechanistic narrative in 2011 by demonstrating that tesamorelin’s visceral adipose reduction correlates with reductions in inflammatory markers, suggesting the metabolic effects extend beyond raw fat-mass changes. Stanley and colleagues8 then extended Tesamorelin research to liver fat (intrahepatic lipid) reduction in a 2014 JAMA trial, demonstrating that the Theratechnologies clinical program continued post-approval into adjacent metabolic endpoints.
Predictors of Treatment Response
Mangili and colleagues16 published a 2015 PLoS ONE pooled-Phase-3 analysis identifying baseline IGF-1, sex, and adiposity as predictors of tesamorelin response. The heterogeneity of response across the registrational population is itself research-context information: studies designed around stabilized-analog pharmacology may select for or stratify on these baseline characteristics. Full single-compound depth on Tesamorelin sits at the Tesamorelin research guide.
Sermorelin: GHRH(1-29)NH2 Fragment and Geref® Dual-NDA History
Sermorelin acetate is the active ingredient in Geref®. The FDA approved an earlier diagnostic formulation in December 1990 under NDA 19-863 (sermorelin acetate 0.05 mg/ampoule for diagnostic evaluation of pituitary GH reserve), followed by the therapeutic formulation on September 26, 1997 under NDA 20-443 (0.5 / 1.0 mg/vial for pediatric idiopathic growth hormone deficiency). EMD Serono notified FDA of voluntary withdrawal in December 2008; the withdrawal was explicitly determined NOT to be for safety or effectiveness reasons — it was a voluntary commercial discontinuation. Apex Laboratory’s research-grade Sermorelin Acetate is classified as a chemical research reagent and is distinct from the previously-approved Geref® formulations.
Foundational Clinical Pharmacology
The Sermorelin lineage in the clinical literature predates either NDA. Vance, Evans, Kaiser, Burke, Rivier, Vale, and Thorner9 published a 1986 Clinical Pharmacology and Therapeutics dose-response study of [Nle27]GHRH(1-29)-NH2 — the sermorelin analog — across intravenous, subcutaneous, and intranasal administration in healthy men. Subcutaneous administration emerged as the route that would later anchor Geref® registrational dosing. The same University of Virginia group built the program that supported the eventual NDAs.
The Geref® Pediatric GHD Registrational Trial
The canonical Geref® pediatric trial was published in the Journal of Clinical Endocrinology and Metabolism by Thorner and colleagues10 in 1996, on behalf of the Geref International Study Group. The international multicenter trial documented that once-daily subcutaneous sermorelin accelerates linear growth in GH-deficient children during the first year of therapy. This was the clinical-trial evidence package that supported the September 26, 1997 FDA approval of the therapeutic Geref® formulation under NDA 20-443.
Older-Adult GH-Axis Restoration
Khorram, Laughlin, and Yen11 published a 1997 Journal of Clinical Endocrinology and Metabolism trial demonstrating that 16 weeks of [Nle27]GHRH(1-29)-NH2 administration in age-advanced men and women restored a more youthful GH/IGF-1 secretory profile. The paper anchors the older-adult GH-axis-restoration paradigm that defines much of Sermorelin’s research-context literature. Walker12 contextualized this paradigm in a 2006 Clinical Interventions in Aging clinical perspective framing GHRH-analog physiologic-pulsatile stimulus as distinct from direct hormone administration. Full single-compound depth on Sermorelin sits at the Sermorelin research guide.
Receptor Pharmacology: Shared GHRH-R Agonism, Different Pharmacokinetic Profiles
Both Tesamorelin and Sermorelin bind the same molecular target — the pituitary-specific growth hormone-releasing hormone receptor (GHRH-R) — first cloned by Mayo3 in 1992 in Molecular Endocrinology. GHRH-R is a class B G-protein-coupled receptor expressed predominantly on pituitary somatotrophs; ligand binding initiates cAMP/PKA signaling that drives growth hormone secretion. Whether the ligand is the full 44-residue Tesamorelin or the 29-residue Sermorelin, receptor identity is the same.
Why Pharmacokinetic Profiles Diverge
The pharmacokinetic divergence between the two compounds traces to one structural fact: the N-terminus. Native GHRH carries a Tyr-Ala N-terminal sequence that is the substrate for DPP-IV cleavage4. Sermorelin retains that Tyr-Ala N-terminus unmodified, so DPP-IV access is preserved and plasma half-life is short (~11–12 minutes). Tesamorelin’s trans-3-hexenoyl modification at the N-terminus blocks DPP-IV, yielding a plasma half-life roughly two to three times longer (~26–38 minutes). Both half-lives remain short relative to dosing intervals, but the difference is sufficient to drive the once-daily registrational dosing structure that Tesamorelin’s Phase 3 program established.
Distinction from Family 2 Ghrelin Mimetics
GHRH-R agonism is one of two pituitary input systems that drive somatotroph GH secretion. The parallel system — the growth hormone secretagogue receptor (GHS-R1a) — was characterized through the GHRP family by Bowers14 in a 1998 Cellular and Molecular Life Sciences retrospective on synthetic GH-secretagogues. Compounds like Ipamorelin and the GHRPs act on the same somatotrophs through GHS-R1a rather than GHRH-R, and their pharmacology is therefore distinct from both Tesamorelin and Sermorelin. The cluster-up GH-axis research peptide pillar covers the full receptor-system taxonomy.
Pulsatile Signaling Preservation vs Direct rhGH Administration
A defining feature of GHRH-analog pharmacology — shared by both Tesamorelin and Sermorelin — is preservation of the endogenous pulsatile signaling logic that governs physiological GH secretion. Walker12 framed this as the central GHRH-analog paradigm in his 2006 clinical perspective: rather than overriding endogenous GH-axis architecture by administering recombinant human growth hormone (rhGH) directly, GHRH-R agonists stimulate the pituitary to release its own GH along the body’s existing pulsatile rhythm, subject to feedback by IGF-1 and somatostatin.
Khorram, Laughlin, and Yen11 demonstrated this paradigm experimentally in older adults: administering a sermorelin analog over 16 weeks restored a more youthful GH/IGF-1 secretory profile while preserving the underlying pulsatility — a contrast with direct rhGH administration, which suppresses endogenous GHRH output via negative feedback. Tesamorelin’s longer half-life modulates the kinetics of stimulus, but the pulsatility-preserving logic is retained: pituitary somatotrophs respond, IGF-1 rises, and feedback regulation continues operating. For research designs anchored to the physiologic GH-axis paradigm rather than to direct hormone replacement, both compounds sit on the same side of this distinction.
Research-Context Use Cases: When Investigators Choose One Over the Other
Because both compounds activate the same receptor and preserve the same pulsatility paradigm, the research-design question is not “which is better” but “which structural and pharmacokinetic profile matches the experimental question.” A few framings:
For studies of stabilized-analog pharmacokinetics or DPP-IV-resistance structure-activity relationships, Tesamorelin’s full-length GHRH(1-44) with N-terminal trans-3-hexenoyl modification is the obvious candidate — the modification is the experimental variable. Mangili and colleagues16 documented baseline-IGF-1, sex, and adiposity heterogeneity in tesamorelin response, suggesting study designs in this domain may benefit from baseline-stratification.
For studies of GHRH(1-29) fragment pharmacology or GH-axis older-adult restoration paradigms, Sermorelin is the foundational reagent — its 29-residue length is the structural feature defining the research lineage from Vance 1986 through Khorram 1997 through Walker 2006.
For studies of multi-day-half-life GHRH-analog kinetics, neither Tesamorelin nor Sermorelin is the primary candidate — CJC-1295 with DAC13 sits in that space with its albumin-binding maleimide modification, characterized by Teichman and colleagues in 2006. The CJC-1295 with DAC research guide covers that compound’s distinctive pharmacology in depth.
For studies of HIV-associated lipodystrophy mechanism or post-registrational metabolic-endpoint extensions, Tesamorelin’s published clinical literature is the deepest, with seven peer-reviewed Phase 3 + post-registration papers cited in this guide. For studies of pediatric or older-adult GH-axis stimulation paradigms, Sermorelin’s Geref-era and post-Geref clinical literature anchors the research-context pattern.
Apex Catalog Availability and Quality Verification
Apex Laboratory carries both Tesamorelin and Sermorelin Acetate as research-grade chemical reagents at ≥99% purity, verified by HPLC and mass spectrometry on every batch and documented in the lab-verified COA archive under the editorial standards framework. Apex’s research-grade Tesamorelin is distinct from the approved Egrifta® / Egrifta SV® pharmaceutical formulations; Apex’s research-grade Sermorelin Acetate is distinct from the previously-approved Geref® formulations. Both compounds, alongside CJC-1295 with DAC, are catalog members within the growth hormone axis research peptide pillar and are accessible through the Apex Research Library under the Growth Hormone Axis Research focus filter.
Research-Grade GHRH Analogs
Tesamorelin
Apex Laboratory Tesamorelin is supplied as a research-grade chemical reagent at ≥99% purity, verified by HPLC and mass spectrometry on every batch. Stabilized full-length GHRH(1-44) analog with N-terminal trans-3-hexenoyl modification; distinct from the FDA-approved Egrifta® / Egrifta SV® pharmaceutical formulations. For in-vitro and preclinical research only — not for human consumption.
View Product →Sermorelin Acetate
Apex Laboratory Sermorelin Acetate is supplied as a research-grade chemical reagent at ≥99% purity, verified by HPLC and mass spectrometry on every batch. GHRH(1-29)NH2 N-terminal fragment of native GHRH; distinct from the previously-approved Geref® formulations. For in-vitro and preclinical research only — not for human consumption.
View Product →CJC-1295 with DAC
Apex Laboratory CJC-1295 with DAC is supplied as a research-grade chemical reagent at ≥99% purity, verified by HPLC and mass spectrometry on every batch. Long-acting GHRH(1-29) analog with maleimide drug-affinity-complex (albumin-binding) extending half-life into the multi-day range. For in-vitro and preclinical research only — not for human consumption.
View Product →Frequently Asked Questions
What is the difference between tesamorelin and sermorelin?
Tesamorelin is a stabilized full-length GHRH(1-44) analog with an N-terminal trans-3-hexenoyl modification conferring DPP-IV proteolytic resistance; Sermorelin is the GHRH(1-29)NH2 N-terminal fragment of native GHRH. Both bind the same GHRH-R receptor on pituitary somatotrophs, but Tesamorelin’s modification yields a longer plasma half-life (~26–38 minutes versus ~11–12 minutes for Sermorelin).
Is tesamorelin stronger than sermorelin?
The compounds are not directly comparable on a “stronger” scale. Tesamorelin and Sermorelin sit at different points in the GHRH-analog structural lineage and at different points in the regulatory-status spectrum. Researchers select between them based on the structural and pharmacokinetic question their study addresses, not on a head-to-head potency comparison.
What are the half-lives of tesamorelin and sermorelin?
Sermorelin has a plasma half-life of approximately 11–12 minutes following subcutaneous administration, limited by DPP-IV cleavage at the N-terminal Tyr-Ala bond. Tesamorelin’s stabilized structure extends plasma half-life to approximately 26–38 minutes, supporting once-daily subcutaneous dosing in the Egrifta® registrational Phase 3 program. Both half-lives remain short relative to dosing intervals.
Were Egrifta® and Geref® both FDA-approved?
Yes, at different points. Egrifta® (tesamorelin) was FDA-approved November 10, 2010 under NDA 22-505 for HIV-associated lipodystrophy in adults; Egrifta SV® reformulation followed in 2019. Geref® (sermorelin acetate) was FDA-approved September 26, 1997 under NDA 20-443 for pediatric growth hormone deficiency, with an earlier December 1990 diagnostic NDA 19-863, and was voluntarily withdrawn from the US market in 2008 for commercial reasons, not safety.
Why is tesamorelin more stable than sermorelin?
DPP-IV cleavage at the N-terminal Tyr-Ala bond rapidly degrades native GHRH and unmodified GHRH(1-29) fragments like Sermorelin. Tesamorelin’s trans-3-hexenoyl N-terminal modification physically blocks DPP-IV access to that bond, extending plasma half-life relative to unmodified GHRH(1-29)NH2. The structural difference is the engineered cap, not the sequence length itself.
How do tesamorelin and sermorelin compare for research applications?
Research selection depends on the question. Tesamorelin is anchored to stabilized-analog pharmacology and HIV-associated lipodystrophy literature with a deep Phase 3 + post-registration evidence base. Sermorelin is anchored to GHRH(1-29) fragment pharmacology, pediatric GHD registrational data, and older-adult GH-axis restoration paradigms. Both are research-grade reagents in the Apex catalog, supplied at ≥99% purity for in-vitro work.
What is the difference between GHRH(1-44) and GHRH(1-29)?
GHRH(1-44) is the full-length 44-residue native human growth hormone-releasing hormone characterized by Guillemin and Rivier groups in 1982. GHRH(1-29) is the synthetic N-terminal 29-residue fragment that retains GHRH-R binding affinity in those first 29 residues. Tesamorelin uses the full 44-residue scaffold with stabilization; Sermorelin uses the 29-residue N-terminal fragment.
Continue Your Research
Researchers building broader Tesamorelin vs Sermorelin context across the Apex library may find the following references useful:
- Growth Hormone Axis Research Peptide Pillar — category umbrella covering GHRH analogs, ghrelin mimetics, and the broader GH-axis research family
- Tesamorelin Research Guide — full single-compound deep-dive on the stabilized GHRH(1-44) analog and Egrifta® registrational program
- Sermorelin Research Guide — full single-compound deep-dive on the GHRH(1-29)NH2 fragment and Geref® registrational history
- CJC-1295 with DAC Research Guide — adjacent long-acting GHRH(1-29) analog with albumin-binding maleimide modification
- Tissue Repair Research Peptide Pillar — lateral pillar covering BPC-157, TB-500, and the tissue-repair family
- GLP-1 / Metabolic Research Peptide Pillar — lateral pillar covering Semaglutide, Tirzepatide, and the broader incretin landscape
- Nootropic and CNS Research Peptide Pillar — lateral pillar covering Selank, Semax, and the CNS research-peptide family
- Sermorelin vs CJC-1295 — sibling GHRH comparison involving Sermorelin and the CJC-1295 lineage
- Ipamorelin vs CJC-1295 — lateral GH-axis comparison across GHRH and ghrelin-mimetic mechanisms
Research Use Disclaimer
This article is provided for educational and research reference purposes only. Tesamorelin, Sermorelin Acetate, CJC-1295 with DAC, and all products sold by Apex Laboratory are intended exclusively for in-vitro laboratory research use and are not for human consumption. Tesamorelin is the active ingredient in Egrifta® (FDA-approved November 10, 2010 under NDA 22-505 for HIV-associated lipodystrophy in adults; Egrifta SV® reformulation 2019); Apex Laboratory’s research-grade Tesamorelin is a chemical research reagent distinct from the approved Egrifta® / Egrifta SV® formulations. Sermorelin acetate was the active ingredient in Geref® (FDA-approved September 26, 1997 under NDA 20-443 for pediatric idiopathic growth hormone deficiency, with an earlier December 1990 diagnostic NDA 19-863); Geref® was voluntarily withdrawn from the US market in 2008 for commercial reasons, not safety. Apex Laboratory’s research-grade Sermorelin Acetate is a chemical research reagent distinct from the previously-approved Geref® formulations. Researchers should consult the primary peer-reviewed literature for trial protocols and findings.
