
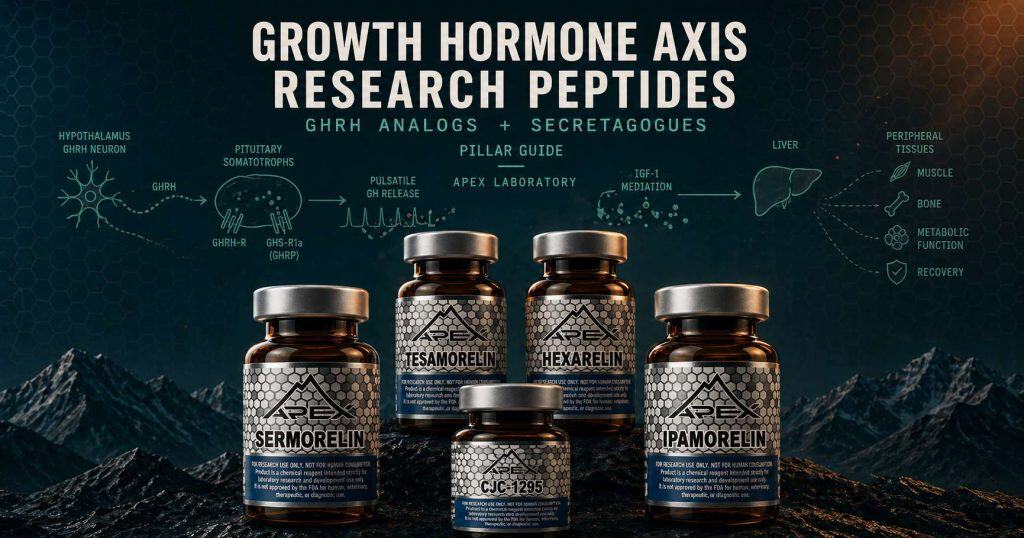
GH-axis research peptides are compounds studied for their effects on the growth hormone signaling cascade — from hypothalamic releasing peptides through pituitary secretagogues to peripheral effectors. They include GHRH-receptor analogs (Sermorelin, Tesamorelin, CJC-1295) and ghrelin-mimetic GHS-R1a agonists (Ipamorelin, GHRP-2, Hexarelin), each acting on a defined receptor pathway documented in primary endocrinology research.
The growth hormone axis is one of the cleanest hierarchical cascades in mammalian endocrinology. Hypothalamic neurons release growth hormone-releasing hormone (GHRH) and somatostatin into the hypophysial portal circulation. Pituitary somatotrophs integrate that stimulus alongside parallel input from the GHS-R1a ghrelin receptor and respond by releasing growth hormone in pulsatile bursts. Hepatic GHR / JAK2 / STAT5 signaling translates circulating GH into insulin-like growth factor 1 (IGF-1). IGF-1 then mediates most of the cascade’s peripheral effects on muscle, bone, adipose, and connective tissue. The fourteen GH-axis research peptides in the Apex Laboratory catalog do not act on the same target — they act on specific nodes of this cascade. Identifying which node a given compound engages is the first analytical question in any GH-axis research design, and it is the organizing question this guide answers.
This guide maps the Apex GH axis peptides catalog along the cascade itself. Five mechanism families are anchored by named-investigator discovery programs and indexed against twenty-two PubMed-verified primary citations. The guide closes with a regulatory-landscape section that distinguishes the two compounds carrying FDA approval history (Tesamorelin’s Egrifta® and Sermorelin’s Geref® lineage) from the twelve research-only catalog members.
Defining the Growth Hormone Axis
Structurally, the growth hormone axis comprises four anatomical levels separated by named molecular handoffs at each transition. At the hypothalamic level, GHRH-secreting neurons in the arcuate nucleus and somatostatin-secreting neurons in the periventricular nucleus drive opposing inputs into the hypophysial portal circulation. Somatostatin acts as the brake, GHRH as the accelerator. At the pituitary level, somatotrophs of the anterior pituitary integrate the portal GHRH signal with a second, parallel input through the growth hormone secretagogue receptor 1a (GHS-R1a). This is the receptor identified in 1999 as the endogenous target of stomach-derived ghrelin. At the hepatic level, pulsatile circulating GH binds the dimeric GH receptor on hepatocytes and activates the JAK2 / STAT5 signaling axis, inducing IGF-1 transcription and release. At the peripheral-tissue level, IGF-1 binds the IGF-1 receptor on skeletal muscle, bone, adipose, and connective tissue. There it mediates most of the proliferative, anabolic, and metabolic actions classically attributed to GH itself.8
Cascade anatomy and molecular handoffs
Two features of this cascade matter for compound-class organization. The first is the two-input pulse-generating logic at the somatotroph level: GHRH-R and GHS-R1a are distinct class-B GPCR systems, and their co-engagement produces synergistic supra-additive GH release rather than additive output. The second is the pulsatile rather than tonic character of the resulting GH secretion. Endogenous GH does not circulate at a steady level; it appears in discrete pulses governed by the hypothalamic GHRH-somatostatin oscillator and modulated by ghrelin input. Compounds engaging either input upstream of the pituitary preserve this physiologic pulsatility; direct hormone administration overrides it.7
Compound classes mapped to cascade nodes
The fourteen GH axis peptides in the Apex catalog distribute across the cascade as follows. Family 1 (Sermorelin Acetate, Tesamorelin, CJC-1295 with DAC, CJC-1295 No DAC) engages the hypothalamus-to-pituitary stimulus by binding GHRH-R on somatotrophs; these are the GHRH analogs that mimic the native hypothalamic signal. Family 2 (Ipamorelin, GHRP-2, GHRP-6, Hexarelin Acetate) provides parallel pituitary input through GHS-R1a. These are the ghrelin mimetics, also called growth hormone secretagogues or GH releasing peptides.
Family 3 (IGF-1 LR3, PEG-MGF) acts at the liver-to-peripheral mediation step, engaging IGF-1 receptor signaling directly or through muscle-stretch-induced splice variants. Family 4 (ACE-031, Follistatin 344) sits adjacent to the canonical cascade in the myostatin and activin pathway, where research interest centers on muscle-physiology crosstalk rather than direct GH-axis stimulation. Family 5 (AOD9604) contains a single compound — a sixteen-amino-acid C-terminal hGH fragment with an adjunct lipolytic mechanism. The catalog also includes a CJC-1295 No DAC + Ipamorelin Blend combination preparation that engages both Family 1 and Family 2 receptor systems simultaneously.
GH Axis Research Peptides at a Glance
- The growth hormone axis runs hierarchically from hypothalamic GHRH and somatostatin through pituitary somatotrophs to hepatic IGF-1 induction and peripheral tissue mediation across muscle, bone, adipose, and connective tissue
- Five mechanism families organize the catalog: GHRH-receptor analogs (Sermorelin, Tesamorelin, CJC-1295), ghrelin mimetics targeting GHS-R1a (Ipamorelin, GHRP-2, GHRP-6, Hexarelin), IGF-1 axis effectors (IGF-1 LR3, PEG-MGF), the myostatin and activin pathway (ACE-031, Follistatin 344), and the adjunct GH-fragment AOD9604
- Tesamorelin is the active ingredient in Egrifta® (FDA-approved November 10, 2010 under NDA 22-505 for HIV-associated lipodystrophy in adults); Apex’s research-grade Tesamorelin is a chemical research reagent distinct from the approved Egrifta® formulation
- Sermorelin’s Geref® was FDA-approved on September 26, 1997 (NDA 20-443) for pediatric growth hormone deficiency with an earlier diagnostic NDA in December 1990; the therapeutic was voluntarily withdrawn from the US market in 2008 for commercial reasons, not safety
- GHRH-receptor agonism on somatotrophs combined with parallel GHS-R1a engagement produces supra-additive GH release — the canonical pharmacological basis for the CJC-1295 No DAC + Ipamorelin Blend combination preparation
- Apex Laboratory supplies all fourteen catalog compounds as research-grade chemical reagents intended exclusively for in-vitro laboratory research, distinct from any approved pharmaceutical formulations
Foundational Discovery Programs
The GH-axis research literature is anchored by a multi-decade scientific genealogy spanning hypothalamic neuroendocrinology, pituitary somatotroph pharmacology, ghrelin biology, and synthetic-analog medicinal chemistry. Four named-investigator programs provide the spine of the field, and the timeline that follows situates each program within the eight milestones that connect 1976 synthetic-peptide work to the contemporary regulatory landscape.
Bowers and Momany at Tulane: synthetic GH-releasing peptides (1976–1984)
Cyril Y. Bowers and Frank A. Momany at Tulane University began synthesizing structural analogs of enkephalins in the mid-1970s and identified, in the process, a small hexapeptide that specifically released growth hormone from the pituitary without engaging opioid receptors. The lineage paper for the synthetic GHRP family is Bowers, Momany, Reynolds, and Hong’s 1984 Endocrinology characterization of the in-vitro and in-vivo activity of the hexapeptide that later became known as GHRP-6.1 Bowers’s 1998 single-author retrospective in Cellular and Molecular Life Sciences synthesizes the family’s progression from GHRP-6 through GHRP-2 and Hexarelin. The retrospective also frames the GHS-R receptor concept that the 1999 ghrelin discovery would later validate at the molecular level.2
Guillemin and Rivier-Vale at the Salk Institute: hypothalamic GHRH characterization (1982)
Two parallel groups at the Salk Institute reported the structure of human GHRH in the same month of 1982. Roger Guillemin’s group, working from a pancreatic islet tumor causing acromegaly, characterized the 44-residue peptide in Science.3 Wylie Vale and Jean Rivier’s parallel group reported the same structural characterization in Nature the following week.4 Both papers were enabled by the unusual abundance of the GHRH peptide in pancreatic-tumor extracts from patients with acromegaly — a tissue source the field had been searching for through the 1970s. The 44-residue GHRH established at Salk in 1982 underwrites every downstream Family 1 GHRH-R analog and remains the structural reference against which Sermorelin, Tesamorelin, and CJC-1295 are designed.
Patchett at Merck: the first oral non-peptide secretagogue (1995)
Arthur A. Patchett, Ravi P. Nargund, and the Merck Research Laboratories medicinal-chemistry program reported the design and biological characterization of L-163,191 — later renamed MK-0677 and ultimately ibutamoren — in PNAS in 1995.5 MK-0677 was the first orally active, non-peptide growth hormone secretagogue characterized in the literature. Its pharmacology established a receptor concept — the growth hormone secretagogue receptor — that anticipated by four years the identification of ghrelin as the endogenous ligand for that same receptor. The Merck program is the proximate source of the GHS-R1a pharmacology now central to the entire ghrelin-mimetic family.
Kojima at NCVC Osaka: ghrelin discovery (1999)
Masayasu Kojima, Hiroshi Hosoda, Kenji Kangawa and colleagues at the National Cardiovascular Center Research Institute in Osaka identified ghrelin in 1999 as the endogenous 28-residue acylated peptide ligand for the orphan GHS-R1a. The acylation modification — n-octanoyl at Ser3 — is essential for receptor activation.6 The Kojima paper closed the loop between Bowers’s synthetic GHRPs from 1976 onward, Patchett’s MK-0677 from 1995, and the endogenous receptor system that the synthetic compounds had been engaging without anyone yet knowing what natural ligand the receptor was waiting for.
-
1976–1984
Bowers and Momany discover synthetic GH-releasing peptides at Tulane
Cyril Y. Bowers and Frank A. Momany at Tulane identify the first synthetic GH-releasing hexapeptides; the canonical 1984 Endocrinology paper characterizes the hexapeptide that becomes GHRP-6, founding the synthetic GH-releasing-peptide lineage. Bowers, Momany, Reynolds, and Hong (1984).
-
1982
Guillemin and Rivier-Vale characterize hypothalamic GHRH at the Salk Institute
Two parallel Salk groups isolate the 44-residue human GHRH peptide from pancreatic-tumor tissue causing acromegaly. Guillemin et al., Science (1982) and Rivier, Spiess, Thorner, and Vale, Nature (1982). The 44-residue structure underwrites every subsequent GHRH-analog development program.
-
1990 / 1997
Sermorelin (Geref®) FDA dual-NDA approvals
Geref® diagnostic formulation (sermorelin acetate 0.05 mg/ampoule) is approved in December 1990 under NDA 19-863 for pituitary GH-reserve assessment. The therapeutic formulation (0.5 / 1.0 mg/vial) is approved on September 26, 1997 under NDA 20-443 for pediatric growth hormone deficiency. Khorram, Laughlin, and Yen (1997) establish the older-adult sermorelin-administration paradigm in J Clin Endocrinol Metab.
-
1995
Patchett at Merck characterizes MK-0677 — the first oral non-peptide secretagogue
Arthur Patchett, Ravi Nargund, and the Merck Research Laboratories team report L-163,191 (later MK-0677, then ibutamoren) in PNAS — the first orally active, non-peptide growth hormone secretagogue. The paper anchors the GHS-R pharmacology that the 1999 ghrelin discovery later validates. Patchett et al. (1995).
-
1999
Kojima et al. identify ghrelin as the endogenous GHS-R1a ligand
Masayasu Kojima and colleagues at NCVC Osaka identify ghrelin as the endogenous 28-residue acylated peptide ligand for the orphan GHS-R1a, with the n-octanoyl modification at Ser3 essential for activity. Kojima, Hosoda, Date, Nakazato, Matsuo, and Kangawa, Nature (1999). Closes the loop between synthetic GHRPs and endogenous receptor biology.
-
2006
Teichman et al. characterize CJC-1295 DAC pharmacokinetics
Steven L. Teichman, with senior author Lawrence A. Frohman, reports the first-in-human pharmacokinetic characterization of CJC-1295 with DAC in J Clin Endocrinol Metab. Single subcutaneous doses produce sustained GH and IGF-1 elevation over six to eleven days, defining the ~8-day half-life that distinguishes the DAC form from the ~30-minute non-DAC form. Teichman et al. (2006).
-
2010
Tesamorelin (Egrifta®) FDA-approved for HIV-associated lipodystrophy
Egrifta® is FDA-approved on November 10, 2010 under NDA 22-505 for the reduction of excess abdominal fat in HIV-infected adults with lipodystrophy. The registrational evidence base is built on Falutz et al., NEJM (2007) and Falutz et al., JCEM (2010) pooled Phase 3 with 52-week safety extension. The first and only currently FDA-approved GHRH analog.
-
2013
Attie et al. report ACE-031 Phase 1; Acceleron program subsequently discontinued
Kenneth Attie and the Acceleron Pharma team report the first-in-human single-ascending-dose study of ACE-031 (ramatercept), a soluble ActRIIB-Fc fusion myostatin antagonist, in Muscle & Nerve. Dose-dependent increases in lean mass and thigh muscle volume are documented. Acceleron subsequently discontinued the development program; the compound is research-only globally. Attie et al. (2013).
Family 1 — GHRH-Receptor Analogs (Sermorelin, Tesamorelin, CJC-1295)
For deeper GH-axis comparisons, see Sermorelin vs CJC-1295, Tesamorelin vs Sermorelin comparison, and Ipamorelin vs CJC-1295.
The first compound family in the GH-axis catalog binds the GHRH receptor on pituitary somatotrophs, mimicking the hypothalamic stimulus while preserving the downstream pulsatile signaling logic of the native cascade. Four catalog members occupy this family — Sermorelin Acetate, Tesamorelin, CJC-1295 with DAC, and CJC-1295 No DAC — and the canonical combination preparation that engages GHRH-R alongside GHS-R1a sits at the family’s closing.
Sermorelin Acetate: GHRH(1-29)NH2 and the Geref® dual-NDA lineage
Sermorelin is the synthetic 29-residue N-terminal fragment of native human GHRH, capped at the C-terminus as a primary amide — GHRH(1-29)NH2. The fragment retains the receptor-binding affinity of the full 44-residue hypothalamic peptide while offering substantially simpler synthesis and characterization. Walker’s clinical review in Clinical Interventions in Aging frames sermorelin within the physiologic-pulsatile-stimulus paradigm that distinguishes GHRH-analog research from direct hormone administration.11 Khorram, Laughlin, and Yen reported in J Clin Endocrinol Metab in 1997 on long-term administration of the [Nle27]GHRH(1-29)NH2 sermorelin analog. Treatment of age-advanced men and women restored a more youthful GH and IGF-1 secretory profile over sixteen weeks.12
Geref® was FDA-approved for pediatric growth hormone deficiency on September 26, 1997 under NDA 20-443. An earlier diagnostic formulation had been approved in December 1990 under NDA 19-863. The therapeutic was voluntarily withdrawn from the US market in 2008 for commercial reasons, not safety. Apex Laboratory’s research-grade Sermorelin is classified as a chemical research reagent and is distinct from the previously-approved Geref® formulations. The detailed Sermorelin research guide covers per-compound pharmacology, structural rationale, and trial-program detail beyond this pillar’s family-level treatment.
Tesamorelin: trans-3-hexenoyl-modified GHRH(1-44) and Egrifta® FDA approval
Tesamorelin is a stabilized full-length GHRH(1-44) analog carrying a trans-3-hexenoyl modification at the N-terminus that confers proteolytic resistance against dipeptidyl peptidase-IV degradation, extending circulating half-life relative to native GHRH. The compound is the active ingredient in Egrifta® (FDA-approved November 10, 2010 under NDA 22-505 for HIV-associated lipodystrophy in adults). Apex Laboratory’s research-grade Tesamorelin is classified as a chemical research reagent and is distinct from the approved Egrifta® formulation.
The registrational evidence base rests on two Falutz-led trials. The pivotal Phase 3 randomized placebo-controlled trial in NEJM in 2007 enrolled 412 HIV-infected patients with abdominal-fat accumulation. Over 26 weeks, 2 mg subcutaneous tesamorelin daily produced a 15.2% reduction in visceral adipose tissue against a 5.0% increase in placebo.9 The pooled analysis in J Clin Endocrinol Metab in 2010 combined the two pivotal Phase 3 trials with a 52-week safety extension. It documented sustained visceral fat reduction with acceptable tolerability across the extended follow-up.10 Egrifta® remains the first and only currently FDA-approved GHRH analog. The dedicated research-grade Tesamorelin product page covers per-compound trial detail, the Egrifta SV® reformulation, and the research-grade-versus-approved-pharmaceutical distinction in greater depth.
CJC-1295 with DAC: drug-affinity-complex albumin-binding technology
CJC-1295 is a tetra-substituted GHRH(1-29) analog (D-Ala2, Gln8, Ala15, Leu27) with an additional N-terminal stabilization. The “with DAC” form carries a maleimidopropionic acid linker that forms a covalent thioether bond with the free Cys34 residue of circulating serum albumin upon administration, generating a long-lived drug-albumin conjugate. Steven L. Teichman and colleagues — with Lawrence A. Frohman, the senior author connecting CJC-1295 to the GHRH-biology lineage — characterized the in-human pharmacokinetics in J Clin Endocrinol Metab in 2006. Single subcutaneous doses produced sustained elevation of GH and IGF-1 secretion over six to eleven days, defining the ~8-day functional half-life that distinguishes the DAC form across the GHRH-analog family.13 The pharmacokinetic extension is the most consequential PK technology in the GH axis. Apex’s CJC-1295 with DAC research guide covers the structural modifications, the DAC chemistry, and the per-compound dosing-study literature in greater depth.
CJC-1295 No DAC: modified GRF(1-29) at ~30-minute half-life
The CJC-1295 No DAC form — also called Modified GRF(1-29) — carries the same four amino-acid substitutions as the DAC form but lacks the maleimidopropionic acid linker. Without the albumin conjugation, the peptide circulates as a free analog with a half-life on the order of thirty minutes — pharmacokinetically aligned with native GHRH and with the pulsatile-stimulus paradigm that Sermorelin established. The two CJC-1295 forms therefore present researchers with structurally similar compounds carrying dramatically different PK profiles. The choice between them organizes around whether a research design calls for sustained tonic GHRH-R engagement or pulsatile stimulus preservation.8
Combination preparations: GHRH-R and GHS-R1a synergy at the pituitary
The CJC-1295 No DAC + Ipamorelin Blend is the canonical Apex combination preparation in this family. The combination engages both GHRH-R (via the CJC-1295 No DAC component) and GHS-R1a (via the Ipamorelin component) on the same somatotroph population. The result is supra-additive GH release rather than additive output — the synergistic pharmacology detailed in the cross-cutting Pulsatility section below. Sigalos and Pastuszak’s 2018 Sexual Medicine Reviews synthesis covers the GH-secretagogue combination context against contemporary clinical literature.22 The companion Ipamorelin research guide covers the GHS-R1a counterpart compound.
Family 2 — Ghrelin Mimetics and GHS-R1a Agonists
Operating on a parallel input channel to the GHRH-R analogs of Family 1, the ghrelin-mimetic compounds bind the growth hormone secretagogue receptor 1a (GHS-R1a) — the same receptor identified by Kojima and colleagues in 1999 as the endogenous target of stomach-derived ghrelin. These are the compounds variously called ghrelin mimetics, growth hormone secretagogues, growth hormone releasing peptides, or GHRPs in the literature. They organize as a family along a single internal axis: receptor selectivity.
Ipamorelin: the first selective GHS-R agonist
Ipamorelin (developmental designation NN703) is a five-residue selective GHS-R1a agonist developed at Novo Nordisk. Karin Raun and colleagues characterized the compound in European Journal of Endocrinology in 1998, reporting that ipamorelin releases growth hormone with potency comparable to GHRP-6 but without the cortisol, prolactin, or ACTH elevations of GHRP-6 and Hexarelin.14 The selectivity profile defines ipamorelin’s position in the family. It sits at the most selective end of the GHS-R1a agonist spectrum and remains the canonical reference compound when researchers require GH release without confounding off-target hormone elevations. The dedicated Ipamorelin research guide covers the selectivity characterization, the receptor-binding studies, and the GHRP-6 comparator data in greater depth.
GHRP-2 (pralmorelin): hexapeptide secretagogue with cortisol and prolactin profile
GHRP-2 — also called pralmorelin or KP-102 — is a hexapeptide derivative of the GHRP-6 lineage with higher GH-releasing potency than GHRP-6 in published characterization studies. The compound carries a documented cortisol and prolactin elevation profile that distinguishes it from ipamorelin’s selectivity. GHRP-2 attribution rides on Bowers and Momany’s 1984 Endocrinology hexapeptide foundation,1 and Bowers’s 1998 Cellular and Molecular Life Sciences retrospective synthesizes the family progression that includes pralmorelin.2
GHRP-6: the Bowers and Momany hexapeptide foundation
GHRP-6 is the original synthetic hexapeptide characterized in Bowers, Momany, Reynolds, and Hong’s 1984 Endocrinology paper as the canonical first member of the synthetic GHRP family.1 GHRP-6 is the historical reference compound against which subsequent GHRPs are characterized; it elevates GH potently but carries documented cortisol, prolactin, and ACTH stimulation alongside an appetite-stimulating effect mediated through GHS-R1a in hypothalamic feeding circuits — the mechanism through which ghrelin itself drives the orexigenic signaling that Kojima’s 1999 paper later mapped onto the same receptor system.
Hexarelin Acetate: Mediolanum and Locatelli pharmacology
Hexarelin (His-D-2-methyl-Trp-Ala-Trp-D-Phe-Lys-NH2) is a six-residue synthetic GH-releasing peptide developed at Mediolanum Farmaceutici in collaboration with Vittorio Locatelli’s group at the University of Milan. Romano Deghenghi and colleagues — with Locatelli as senior author — characterized the compound in Life Sciences in 1994, establishing higher reported GH-releasing potency than GHRP-6 in infant and adult rat models alongside cortisol and prolactin elevation comparable to GHRP-6.15 Hexarelin’s secondary research interest centers on the compound’s CD36-mediated cardiac effects, which sit outside the canonical GHS-R1a / GH-releasing axis but appear in the published literature as a distinct pharmacological context. The product-side reference is Hexarelin Acetate.
Selectivity spectrum: the pharmacological distinction within Family 2
The four catalog ghrelin mimetics distribute along a selectivity spectrum that organizes the family analytically. Ipamorelin sits at the selective end, with minimal cortisol, prolactin, or ACTH elevation per Raun’s characterization. GHRP-6, GHRP-2, and Hexarelin sit progressively toward the less-selective end, with each compound documented to elevate cortisol and prolactin alongside GH. The selectivity question is one of the central pharmacological distinctions within the GHS-R1a agonist family and one of the load-bearing comparison points the cross-cutting Pulsatility section below revisits in synergy-paradigm context.
Family 3 — IGF-1 Axis Effectors
Where Families 1 and 2 act upstream of pituitary GH release, Family 3 compounds engage the cascade at the level of IGF-1 — the hepatic-mediator output that translates pulsatile pituitary GH signaling into peripheral tissue effects on muscle, bone, and connective tissue. Two catalog members occupy this family: a designer IGF-1 analog with reduced binding-protein affinity, and a PEGylated derivative of a muscle-stretch-induced IGF-1 splice variant.
IGF-1 LR3 (Long-R3-IGF-1): designer analog with reduced IGFBP affinity
IGF-1 LR3 — also called Long-R3-IGF-1 — is a recombinant analog of human IGF-1 modified by an N-terminal 13-amino-acid extension and an arginine-for-glutamate substitution at position 3. The structural modifications produce a substantial reduction in binding affinity for the IGF binding proteins, particularly IGFBP-3, the dominant circulating IGF-1 carrier. The reduced-IGFBP-affinity profile prolongs the bioavailability of free, receptor-engagable IGF-1 and was characterized in the foundational comparison study by Frances M. Tomas and colleagues at CSIRO and the University of Adelaide. Tomas et al. reported in Journal of Endocrinology in 1991, comparing full-length IGF-1 with the truncated and extended Long-R3-IGF-1 analog in nitrogen-restricted rats. The LR3 analog produced markedly enhanced effects on nitrogen balance and muscle protein metabolism relative to native IGF-1.16 The 1991 J Endocrinol paper — not the 1992 or 1993 Biochemical Journal mis-cite that propagates through vendor literature — is the canonical structural-pharmacology lineage anchor for IGF-1 LR3 research.
PEG-MGF: PEGylated mechano-growth-factor splice variant
Mechano-growth factor — MGF — is the IGF-1Eb splice variant of the IGF-1 gene, produced through alternative splicing in skeletal muscle following stretch and load. Geoffrey Goldspink’s group at University College London and the Royal Free Hospital cloned and characterized the splice variant in Journal of Muscle Research and Cell Motility in 1996, demonstrating the cloning of an IGF-1 isoform expressed in skeletal muscle subjected to mechanical loading.17 PEG-MGF is the synthetic E-domain peptide of the MGF splice variant conjugated to polyethylene glycol — the PEGylation extends circulating half-life relative to native MGF and produces a stable research compound for muscle-stretch-induced signaling investigation. The two Family 3 compounds therefore engage IGF-1 axis biology at structurally distinct points: IGF-1 LR3 acts as a long-acting full-length analog, PEG-MGF as a PEG-stabilized splice-variant E-domain peptide.
Family 4 — Myostatin and Activin Pathway
Family 4 occupies a structurally distinct position in the GH-axis catalog. Both compounds engage muscle-physiology pathways that run adjacent to, rather than within, the canonical hypothalamus-pituitary-liver-tissue cascade — the activin and myostatin axis is regulated independently of GH secretion and IGF-1 induction, and the catalog inclusion of these compounds reflects research interest in the pathway’s crosstalk with GH-axis-driven anabolic biology rather than direct GHRH-R or GHS-R1a engagement.
ACE-031 (ramatercept): soluble ActRIIB-Fc decoy receptor
ACE-031 — developmental designation ramatercept — is a soluble fusion of the extracellular ligand-binding domain of activin receptor type IIB (ActRIIB) with the Fc domain of human IgG1. The fusion protein binds and sequesters myostatin and related TGF-β superfamily ligands (activin A, GDF-11) in the extracellular space, preventing receptor engagement and downstream Smad2/3 signaling that would otherwise restrict skeletal-muscle growth. Kenneth Attie and the Acceleron Pharma team reported the first-in-human single-ascending-dose Phase 1 trial in Muscle & Nerve in 2013, documenting dose-dependent increases in lean mass and thigh muscle volume in healthy volunteers.18 The Acceleron development program for ACE-031 was subsequently discontinued; the compound is research-only globally with no FDA, EMA, or other regulatory approval anywhere, and no implication of ongoing therapeutic development under any sponsor applies. The product-side reference is ACE-031 1mg.
Follistatin 344: activin and myostatin-sequestering protein
Follistatin 344 is the 344-residue mature isoform of follistatin, a secreted glycoprotein that binds and sequesters activin and myostatin in the extracellular space, antagonizing their engagement with type II activin receptors. Se-Jin Lee and Alexandra C. McPherron at Johns Hopkins reported in PNAS in 2001 the foundational mechanism characterization: follistatin overexpression in skeletal muscle dramatically increases muscle mass through myostatin antagonism, and follistatin-myostatin co-administration in vivo abrogates myostatin’s restrictive signaling.19 Follistatin 344 in research preparations represents the soluble protein form of this mechanism for in-vitro and animal-model investigation. The two Family 4 compounds therefore engage the activin-myostatin pathway at distinct mechanistic levels: ACE-031 as a soluble decoy receptor blocking ligand-receptor engagement, Follistatin 344 as a ligand-sequestering binding protein. The product-side reference is Follistatin 344 1mg.
Family 5 — Adjunct GH-Fragment (AOD9604)
Family 5 contains a single compound — AOD9604, a sixteen-amino-acid C-terminal fragment of human growth hormone corresponding to hGH residues 176-191 (Tyr-hGH-(177-191) in some literature). The fragment retains the C-terminal lipolytic activity of native human GH while losing the somatogenic and diabetogenic activities mediated through the larger N-terminal region of the parent hormone. AOD9604 was developed at Monash University in the 1990s through Frank M. Ng’s group and commercialized through Metabolic Pharmaceuticals.
Margaret Heffernan and colleagues — with Ng as senior author — characterized the lipid-metabolism mechanism in Endocrinology in 2001 across obese mice and beta-3-adrenergic-receptor knock-out mice. They reported that AOD9604’s lipolytic action is not directly mediated through β3-AR despite both compounds producing increased β3-AR expression.20 The β3-AR-independent mechanism establishes AOD9604 as metabolically active through pathways distinct from the catecholamine lipolytic axis. The Bornstein-group hGH C-terminal-fragment lineage at Monash predates and informs the 1990s–2000s AOD9604 program. Ma, Macaulay, Maggs, Armstrong, and Bornstein characterized the synthetic peptide pharmacology related to the C-terminal sequence of human growth hormone in Biochimica et Biophysica Acta in 1982. This is the historical lineage paper for the C-terminal hGH-fragment chemistry that AOD9604 ultimately operationalized.21
AOD9604 also receives coverage in the GLP-1 / metabolic research peptides pillar guide at /glp1-metabolic-research-peptides/ under the adjunct-metabolic family — the dual-context framing reflects the compound’s GH-fragment origin and its lipolytic positioning across both research clusters. The two framings are complementary rather than contradictory: AOD9604 is a GH-fragment in cascade-anatomy terms and an adjunct-metabolic compound in receptor-stoichiometry terms, and the catalog references it through whichever frame the surrounding research design calls for.
Mechanism Family Map — GH-Axis Research Peptides
| Family | Receptor target | Representative compound | Research context | Catalog availability |
|---|---|---|---|---|
| 1 — GHRH-Receptor Analogs | GHRH-R (class B GPCR) on pituitary somatotrophs | Tesamorelin (Egrifta®) / Sermorelin (Geref® lineage) / CJC-1295 with DAC | Tesamorelin Phase 3 HIV-associated lipodystrophy (Falutz 2007 NEJM); CJC-1295 DAC PK ~8-day half-life (Teichman 2006 JCEM) | Sermorelin Acetate / Tesamorelin / CJC-1295 with DAC / CJC-1295 No DAC / CJC-1295 No DAC + Ipamorelin Blend |
| 2 — Ghrelin Mimetics / GHS-R1a Agonists | GHS-R1a (ghrelin receptor) on pituitary somatotrophs | Ipamorelin / Hexarelin Acetate | Ipamorelin selectivity profile (Raun 1998 Eur J Endocrinol); Hexarelin pharmacology (Deghenghi/Locatelli 1994 Life Sci) | Ipamorelin / GHRP-2 / GHRP-6 / Hexarelin Acetate |
| 3 — IGF-1 Axis Effectors | IGF-1R on peripheral tissues; reduced IGFBP affinity | IGF-1 LR3 (Long-R3-IGF-1) / PEG-MGF | IGF-1 LR3 designer analog with reduced IGFBP affinity (Tomas 1991 J Endocrinol); MGF stretch-induced splice variant (Yang/Goldspink 1996) | IGF-1 LR3 / PEG-MGF (2mg) |
| 4 — Myostatin and Activin Pathway | ActRIIB soluble decoy / activin and myostatin sequestration | ACE-031 (ramatercept) / Follistatin 344 | ACE-031 Phase 1 (Attie 2013 Muscle Nerve; Acceleron program discontinued); follistatin–myostatin antagonism (Lee & McPherron 2001 PNAS) | ACE-031 (1mg) / Follistatin 344 (1mg) |
| 5 — Adjunct GH-Fragment | β3-AR-independent lipolytic mechanism | AOD9604 (hGH 176-191) | AOD9604 lipid metabolism in β3-AR knock-out mice (Heffernan 2001 Endocrinology); Bornstein-lineage hGH C-terminal pharmacology (Ma et al. 1982) | AOD9604 |
The mechanism family map indexes the five families along their cascade engagement points. Rows trace the cascade from upstream pituitary stimulation (Families 1 and 2) through downstream IGF-1 axis mediation (Family 3) to adjacent muscle-physiology and adjunct lipolytic pathways (Families 4 and 5). The combination preparation in row 1 engages both Family 1 GHRH-R and Family 2 GHS-R1a inputs simultaneously on the same somatotroph population — the synergy paradigm developed in the Pulsatility section below.
Pulsatility, Selectivity, and Pituitary Reserve
Three concepts run cross-cutting through the five-family catalog and explain why GH-axis research design organizes around them rather than around any single compound’s potency: pulsatility, selectivity, and pituitary reserve. Each concept connects the family-level pharmacology of the catalog to the underlying cascade biology and frames the analytical questions a researcher carries into compound selection.
Pulsatile versus tonic signaling
Endogenous growth hormone secretion is pulsatile, not tonic. Veldhuis, Keenan, and Pincus’s 2008 Endocrine Reviews synthesis on the analytical methods for pulsatile hormone secretion — the canonical methodological reference for deconvolution analysis of GH and other pulsatile hormones — formalizes the framework researchers use to characterize axis-active compound effects against the native pulsatile pattern.7 GHRH analogs (Family 1) and ghrelin mimetics (Family 2) preserve the pulsatile-stimulus paradigm by acting upstream of the pituitary — the somatotrophs continue to integrate the exogenous stimulus into the native oscillator’s pulse-generating logic. Direct hormone administration, by contrast, overrides physiologic pulsatility, presenting tissues with a tonic GH signal categorically different from the native cascade output. The pulsatility distinction is one of the central reasons the GH-axis cluster organizes around upstream-stimulus compounds rather than around recombinant GH itself.
GHS-R1a selectivity and off-target hormone profiles
The Family 2 selectivity spectrum, introduced above, recurs as a cross-cutting analytical question. Ipamorelin’s minimal cortisol, prolactin, and ACTH elevation profile — the selectivity characterization Raun and colleagues established as the defining property of the first selective GHS-R agonist14 — sits at one end of the family’s spectrum. GHRP-6, GHRP-2, and Hexarelin sit progressively toward the less-selective end, with each compound documented to elevate cortisol and prolactin alongside GH at varying magnitudes. Selectivity is therefore a research-design parameter rather than a per-compound property in isolation: research models requiring clean isolation of GH-axis signaling without confounding HPA-axis or lactotroph activation favor the selective end of the spectrum, while research questions specifically engaging the broader hypothalamic-pituitary integration may benefit from less-selective compounds.
GHRH-R + GHS-R1a synergy and the combination paradigm
GHRH and ghrelin (and the synthetic GHRPs that mimic ghrelin’s GHS-R1a engagement) activate distinct receptors on the same pituitary somatotroph population. They produce supra-additive — synergistic — GH release in combination, rather than the additive output that two parallel agonists at independent receptor systems might naively predict. The synergy reflects the integrated signaling logic of the somatotroph itself: GHRH-R drives cAMP elevation through Gαs, while GHS-R1a engages Gαq / phospholipase C and intracellular calcium mobilization, and the two pathways converge on GH exocytosis with multiplicative rather than additive output. Sigalos and Pastuszak’s 2018 review covers the combination context against contemporary clinical-research literature.22 The CJC-1295 No DAC + Ipamorelin Blend is the canonical Apex catalog operationalization of this synergy paradigm, and the GHRH vs GHRP mechanism distinction underlying the combination is one of the most-asked questions in the cluster’s research literature. Frohman and Kineman’s 2002 Trends in Endocrinology and Metabolism synthesis of GHRH biology — covering pituitary development, somatotroph hyperplasia, and the broader GHRH-receptor pharmacology that the synergy paradigm presupposes — provides the receptor-pharmacology foundation for this combination-research approach.8
Reading the Regulatory Landscape
Of the fourteen GH-axis research peptides covered in this guide, only two carry regulatory-approval history. Tesamorelin is currently FDA-approved; Sermorelin was previously FDA-approved and was voluntarily withdrawn from the US market in 2008. The remaining twelve compounds are research-only globally — no FDA, EMA, NMPA, or other regulatory approval anywhere — and the regulatory framing for each compound must be applied with per-jurisdiction precision matching the Cerebrolysin research guide precedent.
Tesamorelin (Egrifta®): the only currently FDA-approved GHRH analog
Tesamorelin is the active ingredient in Egrifta® (FDA-approved November 10, 2010 under NDA 22-505 for HIV-associated lipodystrophy in adults); Apex Laboratory’s research-grade Tesamorelin is classified as a chemical research reagent and is distinct from the approved Egrifta® formulation. Theratechnologies is the sponsor of record. A reformulated single-vial Egrifta SV® was FDA-approved in 2019, and a more recent F8-reformulated Egrifta WR® has been approved within the last several years. The registrational evidence base — Falutz et al. NEJM 2007 and Falutz et al. J Clin Endocrinol Metab 2010 — is detailed in the Family 1 section above.910
Sermorelin (Geref®): the dual-NDA withdrawal lineage
Geref® was FDA-approved for pediatric growth hormone deficiency on September 26, 1997 (NDA 20-443; an earlier diagnostic formulation had been approved in December 1990 under NDA 19-863). The therapeutic was voluntarily withdrawn from the US market in 2008 for commercial reasons, not safety. Apex Laboratory’s research-grade Sermorelin is classified as a chemical research reagent and is distinct from the previously-approved Geref® formulations. The withdrawal record — EMD Serono’s December 2008 notification to FDA, published in 74 FR 23407 on May 19, 2009 with effective date June 18, 2009 — explicitly determined that withdrawal was not for safety or effectiveness reasons. The regulatory distinction matters for editorial precision; vendor-literature shorthand commonly conflates it. The Walker and Khorram clinical-program papers cited above anchor the trial-program literature underlying the 1997 therapeutic NDA.1112
Research-only globally: the remaining twelve compounds
CJC-1295 with DAC, CJC-1295 No DAC, Ipamorelin, GHRP-2, GHRP-6, Hexarelin Acetate, IGF-1 LR3, PEG-MGF, ACE-031, Follistatin 344, AOD9604, and the CJC-1295 No DAC + Ipamorelin Blend combination preparation carry no FDA, EMA, NMPA, or other regulatory approval anywhere globally. ACE-031 specifically: the Acceleron development program has been discontinued, and no implication of ongoing therapeutic development under any sponsor applies. The research-only framing for the entire twelve-compound group is uniform — the compounds are research-grade chemical reagents intended exclusively for in-vitro laboratory research.
Sourcing Research-Grade Growth Hormone Peptides
Researchers sourcing growth hormone peptides for laboratory work navigate a market with significant quality variance. Apex Laboratory’s research-grade GH-axis catalog spans the five mechanism families documented above. The flagship trio — Sermorelin Acetate, the CJC-1295 No DAC + Ipamorelin Blend combination preparation, and Tesamorelin — covers the cascade’s pituitary-stimulus level, the GHRH-R + GHS-R1a synergy paradigm, and the only currently FDA-approved GHRH analog as a research-grade reagent distinct from the approved pharmaceutical formulation. The full Apex Research Library indexes this pillar alongside lateral pillars on tissue repair research peptides and CNS research peptides, and the editorial standards and lab-verified hubs document the COA, HPLC, and mass-spectrometry verification framework that Apex’s research-grade discipline rests on. Procedural references for laboratory use — the reconstitution guide, the peptide storage guide, the how to read a COA guide, the HPLC purity testing guide, and the peptide dosing calculator guide — provide the research-context operational documentation that GH-axis compound work calls on.
Flagship trio — research-context catalog presentation
Catalog GH-Axis Research Peptides
Sermorelin Acetate
GHRH(1-29)NH2 — synthetic 29-residue N-terminal GHRH analog. The foundational compound for studying physiological GH-axis stimulation; the active ingredient in the previously-approved Geref® dual-NDA formulations (1990 diagnostic, 1997 therapeutic, voluntarily withdrawn 2008).
View research-grade SermorelinCJC-1295 No DAC + Ipamorelin Blend
Combination GHRH analog + selective ghrelin mimetic. The canonical GHRH-R + GHS-R1a synergy preparation engaging both pituitary stimulus pathways simultaneously on somatotrophs; supra-additive GH release per Sigalos & Pastuszak 2018 review.
View research-grade combination blendTesamorelin
Stabilized trans-3-hexenoyl-modified GHRH(1-44) analog. The active ingredient in Egrifta® (FDA-approved November 10, 2010 for HIV-associated lipodystrophy); Apex’s research-grade Tesamorelin is a chemical research reagent distinct from the approved Egrifta® formulation.
View research-grade TesamorelinCatalog context for adjacent GH-axis research reagents also includes IGF-1 LR3.
Frequently Asked Questions
What are growth hormone peptides?
Growth hormone peptides are synthetic compounds that engage specific nodes of the hypothalamus-pituitary-liver-tissue cascade rather than the GH receptor directly. The Apex catalog covers fourteen such compounds across five mechanism families: GHRH-receptor analogs, ghrelin mimetics targeting GHS-R1a, IGF-1 axis effectors, the myostatin and activin pathway, and the adjunct GH-fragment AOD9604.
What is the difference between GHRH analogs and ghrelin mimetics?
GHRH analogs (Family 1: Sermorelin, Tesamorelin, CJC-1295) bind the GHRH receptor on pituitary somatotrophs, mimicking the native hypothalamic stimulus. Ghrelin mimetics (Family 2: Ipamorelin, GHRP-2, GHRP-6, Hexarelin) bind GHS-R1a, providing parallel pituitary input. Both converge on GH release; combination engagement produces supra-additive output rather than additive.
Are any GH-axis peptides FDA-approved?
Tesamorelin is the active ingredient in Egrifta® (FDA-approved November 10, 2010 under NDA 22-505 for HIV-associated lipodystrophy in adults). Sermorelin’s Geref® was FDA-approved September 26, 1997 (NDA 20-443) for pediatric growth hormone deficiency, with an earlier December 1990 diagnostic NDA, and was voluntarily withdrawn from the US market in 2008 for commercial reasons, not safety. The remaining twelve catalog compounds are research-only globally.
What is CJC-1295 DAC technology?
DAC is the drug-affinity-complex linker — a maleimidopropionic acid moiety that forms a covalent thioether bond with serum albumin’s free Cys34 residue. The conjugation extends circulation dramatically. Teichman et al. (2006) characterized sustained GH and IGF-1 elevation over six to eleven days, defining the ~8-day half-life that distinguishes the DAC form from the ~30-minute non-DAC form.
What are the IGF-1 axis peptides used in research?
The Apex catalog covers two IGF-1 axis effectors. IGF-1 LR3 (Long-R3-IGF-1) — characterized by Tomas et al. in 1991 — is a designer analog with an N-terminal extension and Arg3 substitution producing reduced IGFBP affinity and prolonged free IGF-1 bioavailability. PEG-MGF — Yang and Goldspink 1996 — is a PEGylated derivative of the IGF-1Eb splice variant.
What is the most selective ghrelin mimetic in the Apex catalog?
Ipamorelin is the most selective GHS-R1a agonist in the catalog. Raun and colleagues at Novo Nordisk characterized the compound in European Journal of Endocrinology in 1998, releasing GH with potency comparable to GHRP-6 but without the cortisol, prolactin, or ACTH elevations of GHRP-6 and Hexarelin.
How do researchers approach GH-axis pulsatility in study design?
Endogenous GH secretion is pulsatile, not tonic, per Veldhuis, Keenan, and Pincus’s 2008 Endocrine Reviews methodological synthesis on deconvolution of pulsatile hormone secretion. Axis-active compounds (GHRH analogs and ghrelin mimetics) preserve pulsatile-stimulus signaling and pituitary reserve by acting upstream of the pituitary; this distinguishes their research applications categorically from direct hormone administration, which overrides physiologic pulsatility.
Continue Your Research
Researchers continuing into per-compound depth will find dedicated guides for each Family 1 GHRH-R analog and the canonical Family 2 ghrelin mimetic, alongside the lateral pillar references that situate the GH-axis cluster within the broader Apex research-content architecture.
- Sermorelin research guide — the foundational GHRH(1-29)NH2 compound with Geref® dual-NDA regulatory history
- research-grade Tesamorelin product page — the only currently FDA-approved GHRH analog (Egrifta® November 2010)
- CJC-1295 with DAC research guide — the ~8-day half-life GHRH analog with drug-affinity-complex albumin-binding chemistry
- Ipamorelin research guide — the first selective GHS-R1a agonist with minimal cortisol and prolactin elevation
- Tissue repair research peptides pillar — the lateral cluster covering BPC-157, TB-500, GHK-Cu, and the broader tissue-recovery research-peptide catalog
- CJC-1295 Research Guide
- AOD9604 Research Guide
- BPC-157 Research Guide
- GHK-Cu Research Guide
- TB-500 (Thymosin Beta-4) Research Guide
The forthcoming GLP-1 / metabolic research peptides pillar at /glp1-metabolic-research-peptides/ covers AOD9604 in adjunct-metabolic context as the cross-cluster bridge from this guide’s Family 5 treatment.
Research Use Disclaimer
This article is provided for educational and research reference purposes only. The fourteen growth hormone peptides covered in this guide — Sermorelin Acetate, Tesamorelin, CJC-1295 with DAC, CJC-1295 No DAC, Ipamorelin, GHRP-2, GHRP-6, Hexarelin Acetate, IGF-1 LR3, PEG-MGF (2mg), ACE-031 (1mg), Follistatin 344 (1mg), AOD9604, and the CJC-1295 No DAC + Ipamorelin Blend combination preparation — are supplied by Apex Laboratory as research-grade chemical reagents intended exclusively for in-vitro laboratory research. Tesamorelin is the active ingredient in Egrifta® (FDA-approved November 10, 2010 under NDA 22-505 for HIV-associated lipodystrophy in adults); Apex’s research-grade Tesamorelin is a chemical research reagent distinct from the approved Egrifta® formulation. Geref® was FDA-approved for pediatric growth hormone deficiency on September 26, 1997 (NDA 20-443; an earlier diagnostic formulation had been approved in December 1990 under NDA 19-863), and the therapeutic was voluntarily withdrawn from the US market in 2008 for commercial reasons, not safety; Apex’s research-grade Sermorelin is a chemical research reagent distinct from the previously-approved Geref® formulations. The remaining twelve growth hormone peptides carry no FDA, EMA, NMPA, or other regulatory approval anywhere globally and are research-only compounds. None of the fourteen catalog products is intended for human or veterinary use, diagnostic application, or therapeutic administration.
