
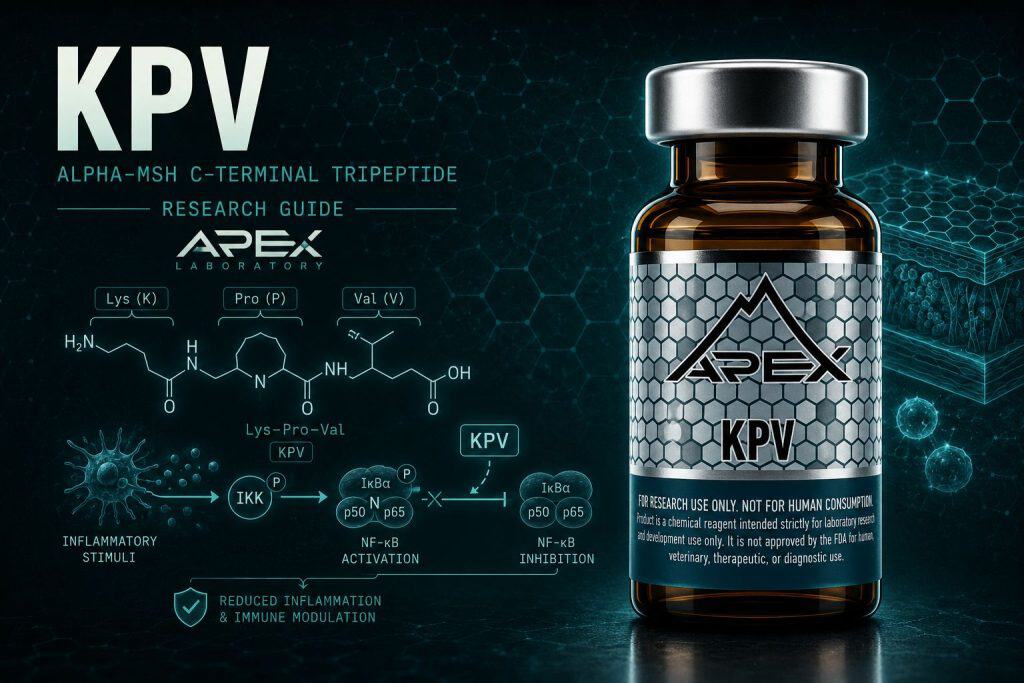
The KPV peptide is a tripeptide of lysine, proline, and valine (Lys-Pro-Val) that corresponds to the C-terminal fragment, residues 11 to 13, of alpha-melanocyte-stimulating hormone (alpha-MSH). Research literature characterizes it as an anti-inflammatory melanocortin-derived peptide that modulates NF-kappaB and MAP-kinase signaling and reduces pro-inflammatory cytokine output in intestinal and other epithelial models, while lacking the pigmentary activity associated with the full-length alpha-MSH hormone.
Alpha-melanocyte-stimulating hormone (alpha-MSH) is a thirteen-residue melanocortin peptide with the sequence SYSMEHFRWGKPV, and within that sequence sits a much smaller molecule that has become a research subject in its own right. KPV — the C-terminal tripeptide of lysine, proline, and valine occupying residues 11 to 13 — is the minimal fragment that, in published preclinical work, retains much of the parent hormone’s anti-inflammatory signaling while shedding the pigmentary activity that characterizes the full melanocortin.[1] That separation of an anti-inflammatory signal from a pigmentary one is the central reason the isolated tripeptide became a focus of melanocortin research.[2]
This guide summarizes the KPV research literature for laboratory context — its melanocortin lineage, its NF-κB-modulating mechanism, the PepT1 transporter route by which it enters intestinal cells, and the colitis and epithelial models in which it has been studied. KPV sits within the broader Apex tissue-repair research cluster, and it is supplied strictly as a research-grade chemical reagent for in-vitro and preclinical investigation — not as a drug, dietary product, or therapy for human or veterinary use.
KPV Peptide at a Glance
- KPV is a tripeptide — Lys-Pro-Val (K-P-V) — corresponding to residues 11–13 at the C-terminus of alpha-melanocyte-stimulating hormone (alpha-MSH, SYSMEHFRWGKPV).
- It has a molecular weight of 342.43 g/mol, molecular formula C16H30N4O4, and CAS number 67727-97-3, all confirmed against PubChem CID 125672.
- Reviews attribute much of the anti-inflammatory activity of alpha-MSH to the C-terminal KPV motif, which is one reason researchers study the isolated tripeptide rather than the full hormone.
- In preclinical models KPV is reported to inhibit NF-κB and MAP-kinase signaling at nanomolar concentrations and to reduce pro-inflammatory cytokine output in intestinal and epithelial cells.
- KPV is distinguished from full-length alpha-MSH by its reported lack of pigmentary action, because it lacks the sequence motif required to bind known melanocortin receptors.
- KPV has no FDA-, EMA-, or other approved formulation anywhere; Apex supplies it strictly as a research-grade chemical reagent at ≥99% purity for in-vitro and preclinical use only.
KPV (Lys-Pro-Val)
What Is the KPV Peptide? The C-Terminal Tripeptide of Alpha-MSH
KPV is a tripeptide composed of three amino acids — lysine, proline, and valine, in that order (Lys-Pro-Val, single-letter K-P-V). It carries a molecular weight of 342.43 g/mol and a molecular formula of C16H30N4O4, with CAS number 67727-97-3, values that are confirmed against PubChem CID 125672. Its defining structural feature is positional: it is the carboxy-terminal fragment, residues 11 through 13, of alpha-melanocyte-stimulating hormone, whose full sequence is SYSMEHFRWGKPV.[1]
A three-amino-acid melanocortin-derived fragment
Where full-length alpha-MSH and the longer melanocortins engage cell-surface melanocortin receptors, KPV is studied in the literature as an anti-inflammatory melanocortin-derived peptide whose activity is largely characterized as receptor-independent. Reviews of the alpha-MSH family describe most of the parent hormone’s anti-inflammatory activity as attributable to this terminal KPV motif, which is precisely why researchers have isolated and studied the tripeptide as a simpler experimental tool than the thirteen-residue hormone.[3]
Why a tripeptide attracts research interest
A short, defined three-residue sequence is attractive experimentally for several reasons: it is structurally simple, chemically tractable, and amenable to identity confirmation by mass spectrometry. The trade-off is that small peptides are enzymatically labile, a handling consideration addressed later in this guide. The authoritative Endocrine Reviews survey of alpha-MSH and related tripeptides frames KPV as a delineated alternative to the full hormone specifically because it preserves the anti-inflammatory effect while avoiding pigmentary action.[2]
From Alpha-MSH to a Three-Amino-Acid Fragment: The Melanocortin Lineage
To understand why KPV is studied at all, it helps to start with its parent. Alpha-MSH is one of several melanocortin peptides cleaved from the precursor protein pro-opiomelanocortin (POMC). Cutuli and colleagues, in their characterization of melanocortin peptides, set out the full alpha-MSH(1–13) sequence as SYSMEHFRWGKPV and explicitly identify KPV as its carboxy-terminal tripeptide spanning residues 11 to 13.[1] That sequence relationship is the lineage anchor for everything that follows.
POMC, alpha-MSH, and the C-terminal motif
The melanocortin system is best known for the pigmentary and energy-balance roles of alpha-MSH acting through melanocortin receptors. In parallel, an immunology-focused literature developed around the observation that alpha-MSH and its related peptides modulate inflammatory signaling. Luger and colleagues, reviewing this body of work, situate alpha-MSH and its C-terminal related peptides — including KPV — within immune-system anti-inflammatory signaling, describing effects on NF-κB activation, adhesion molecules, chemokine receptors, and pro-inflammatory cytokine production.[4]
Why the C-terminal tripeptide became a research focus
The decisive observation, repeated across reviews, is that the anti-inflammatory activity of alpha-MSH does not require the whole molecule. Luger and colleagues state that most of the anti-inflammatory activity of alpha-MSH can be attributed to its C-terminal tripeptide KPV.[3] Once it was clear that the immunomodulatory signal localized to the terminal three residues, the tripeptide itself became the practical experimental handle — smaller, easier to synthesize and verify, and free of the receptor-binding motif that drives pigmentation. KPV is one of several reagents in the Apex tissue-repair research cluster studied for inflammation-modulating signaling.
Anti-Inflammatory Signaling Without Pigmentary Activity
The single most distinctive feature of KPV in the research literature is the dissociation of two properties that are joined in the parent hormone: anti-inflammatory signaling and pigmentary action. This is the structural and pharmacological rationale that justifies studying the fragment rather than alpha-MSH itself.
KPV vs Full-Length Alpha-MSH: Fragment vs Parent Hormone
| Attribute | KPV (Lys-Pro-Val) | Alpha-MSH (full-length) |
|---|---|---|
| Length | 3 amino acids (residues 11–13) | 13 amino acids (SYSMEHFRWGKPV) |
| Melanocortin-receptor binding | Lacks the required binding motif | Binds melanocortin receptors (MC1R–MC5R) |
| Pigmentary action | Reported absent | Present (drives melanogenesis) |
| Reported anti-inflammatory mechanism | Largely receptor-independent; NF-κB suppression | Receptor-mediated plus C-terminal contribution |
| cAMP response | No cAMP rise reported | Receptor-coupled cAMP signaling |
| Regulatory status | Research-only; no approved formulation | Research-only as a reagent; no KPV-type drug approval |
Lacking the melanocortin-receptor binding motif
Brzoska and colleagues, in a review of alpha-MSH-related peptides beyond the pharmacophore, state that KPV lacks the entire sequence motif required to bind any of the known melanocortin receptors, yet retains almost all of the anti-inflammatory capacity of the full hormone while displaying a lack of pigmentary action.[5] The same review is candid that the exact KPV signaling mechanism remains incompletely characterized — a hedge that this guide preserves throughout.
Why pigmentation is decoupled from anti-inflammatory effect
The authoritative Endocrine Reviews treatment makes the motivation explicit: a key obstacle to using alpha-MSH is its pigmentary effect, and the C-terminal tripeptide KPV has been delineated as an alternative precisely because it preserves the anti-inflammatory effect but lacks pigmentary action.[2] Mechanistically, pigmentation in the melanocortin system runs through receptor-mediated cAMP signaling; because KPV does not engage that route (a point detailed in the comparative section below), the pigmentary arm is simply not activated.[6] These are characterizations from preclinical work and are not clinical claims.
NF-kB and Pro-Inflammatory Cytokine Modulation in Research Models
If KPV does not work primarily through melanocortin receptors, how is its anti-inflammatory effect described mechanistically? The recurring answer in the literature centers on the transcription factor NF-κB and the cytokine programs it controls.
KPV uptake via PepT1 → receptor-independent NF-κB suppression
In gut research models, KPV enters intestinal epithelial and immune cells through the di/tripeptide transporter PepT1. Inside the cell, published preclinical work describes a largely receptor-independent anti-inflammatory mechanism: at nanomolar concentrations KPV inhibits NF-κB and MAP-kinase signaling, and in airway-epithelial studies it undergoes nuclear import, stabilizes IκB-alpha, and suppresses nuclear translocation of the p65RelA NF-κB subunit via the importin-alpha binding site. The downstream effect is reduced pro-inflammatory cytokine output, including TNF-alpha, without engaging the melanocortin receptors responsible for pigmentation. All steps are characterized in cell and animal systems. Dalmasso et al. (2008), Gastroenterology.
Nanomolar NF-kB and MAP-kinase inhibition
The cornerstone mechanistic study, by Dalmasso and colleagues, reported that in intestinal epithelial and immune cell models KPV inhibits NF-κB and MAP-kinase signaling at nanomolar concentrations and reduces the secretion of pro-inflammatory cytokines.[7] The nanomolar potency is notable: it indicates the effect is not a nonspecific high-concentration artifact but a defined signaling interaction in the cited cell systems.
Receptor-independent blockade of p65RelA nuclear import
A more granular molecular account comes from Land, working in human bronchial epithelial cells, who reported that KPV dose-dependently inhibits NF-κB activity along with MMP-9, IL-8, and eotaxin. The proposed mechanism is receptor-independent: KPV undergoes nuclear import, stabilizes IκB-alpha, and suppresses nuclear translocation of the p65RelA NF-κB subunit through interaction with the importin-alpha binding site — a route described as distinct from the MC3R-mediated signaling of gamma-MSH.[8]
Cytokine and TNF-alpha downregulation
Downstream of NF-κB suppression, the cited models report reduced output of pro-inflammatory mediators. Work on targeted colonic delivery, for example, described downregulation of TNF-alpha in a mouse ulcerative-colitis model alongside accelerated mucosal healing.[9] It bears emphasizing that the literature is not unanimous on a single mechanism — some reports describe residual melanocortin-receptor interaction — so the receptor-independent NF-κB account is best read as the dominant, but not exclusive, proposal.[4]
PepT1-Mediated Epithelial Uptake: How KPV Enters Intestinal Cells
A peptide that acts on intracellular targets such as the NF-κB machinery must first get inside the cell. For KPV in the gut, the literature identifies a specific route: the di- and tripeptide transporter PepT1.
The di/tripeptide transporter PepT1
Dalmasso and colleagues reported that KPV is taken up via PepT1, which is expressed in intestinal epithelial cells and in immune cells, providing a transport mechanism by which the tripeptide reaches its intracellular site of action.[7] PepT1 normally handles small di- and tripeptides as part of nutrient absorption, and KPV — being a tripeptide — fits that substrate profile.
PepT1-knockout abolishes the effect
The clearest demonstration that this transport route is functionally necessary comes from Viennois and colleagues, who studied KPV in a murine colitis-associated-cancer model. KPV reduced carcinogenesis in wild-type mice but had no such effect in PepT1-knockout mice, establishing that KPV’s reported action in that model is PepT1-dependent.[10] This transporter dependence is well-supported in gut models specifically; it should not be assumed to generalize uniformly to every tissue, since epithelial uptake routes differ across organs. Researchers reconstituting the peptide for uptake studies may consult the Apex guide on how to reconstitute peptides.
KPV in Intestinal and Colitis Research Models
The largest and most coherent body of KPV research is in animal models of intestinal inflammation, where the NF-κB mechanism and the PepT1 uptake route come together in measurable outcomes.
DSS, TNBS, and transfer colitis models
Kannengiesser and colleagues evaluated KPV across multiple murine inflammatory-bowel-disease models, reporting reduced inflammation, less weight loss, lower histologic infiltrate, and decreased myeloperoxidase activity in dextran-sodium-sulfate (DSS) colitis and in CD45RB-high transfer colitis. Notably, the effect was at least partially independent of the MC1 receptor: efficacy was retained in mice with a nonfunctional MC1 receptor.[11] In the foundational Dalmasso work, orally administered KPV reduced both DSS- and TNBS-induced colitis in mice.[7]
The colitis-associated-cancer model
The Viennois study extended the colitis literature into a colitis-associated-cancer (AOM/DSS) model, where KPV reduced tumorigenesis in a PepT1-dependent manner.[10] Reported endpoints across these studies — histologic injury, myeloperoxidase activity as a neutrophil marker, weight recovery, and cytokine expression — are standard preclinical inflammation readouts. Every one of these findings is a result in mice or isolated cells; none has been established in humans, and none should be read as evidence of efficacy in any clinical sense.
Targeted Delivery Systems and Oral Bioavailability Research
A practical obstacle to studying any small peptide in vivo is delivering it intact to the target tissue. A distinct strand of KPV research has therefore focused on engineered delivery systems rather than the peptide alone.
Nanoparticle and hydrogel colonic targeting
Xiao and colleagues described KPV as a naturally occurring tripeptide that attenuates the inflammatory responses of colonic cells, and developed hyaluronic-acid-functionalized nanoparticles to deliver it specifically to colonic epithelial cells and macrophages. In a mouse ulcerative-colitis model, this targeted delivery accelerated mucosal healing and downregulated TNF-alpha.[9] The appeal of such systems is that they aim to concentrate the peptide where it is needed while limiting systemic exposure.
The proteolytic-lability rationale for delivery engineering
Why engineer delivery at all? Songok and colleagues spelled out the underlying problem: peptide drugs, including KPV, are susceptible to enzymatic degradation and rapid elimination, which motivated their work on structurally modified, glycoalkylated KPV analogs that showed improved stability toward proteolytic enzymes.[12] The same lability that drives delivery-system research is also why identity and integrity verification matter when handling the reagent, a theme returned to in the quality section.
KPV Compared to Full-Length Melanocortin Agonists
Because KPV is a fragment of a receptor-active hormone, the most informative comparisons are pharmacological: how does the tripeptide behave relative to the full-length and core melanocortin agonists from which it derives?
No cAMP rise, SHU9119-insensitive, active in MC1-R-null mice
Getting and colleagues dissected the anti-inflammatory effects of the core and C-terminal melanocortin peptides and reported three findings that together separate KPV from classical melanocortin-receptor agonism: KPV did not increase cAMP, its activity was not blocked by the MC3/4-receptor antagonist SHU9119, and the effect was retained in recessive-yellow mice that lack a functional MC1 receptor.[6] On that basis the authors concluded KPV is unlikely to act through melanocortin receptors, more probably acting via interference with interleukin-1-beta signaling.
A different molecular entry point onto an overlapping anti-inflammatory program
The Brzoska review reinforces this picture: lacking the receptor-binding motif entirely, KPV nonetheless retains almost all of the anti-inflammatory capacity of the full hormone.[5] In other words, the tripeptide and the full melanocortins appear to converge on overlapping anti-inflammatory outcomes through distinct molecular routes — the full agonists through receptor-mediated signaling, KPV through a largely receptor-independent, NF-κB-directed mechanism. This is a comparison of research pharmacology, not of approved therapies. Researchers building a comparative tissue-repair reagent panel may also review BPC-157 versus GHK-Cu for adjacent mechanism contrasts.
Breadth of KPV Research Beyond the Gut: Skin, Airway, and Antimicrobial Models
Although the intestinal literature is the deepest, KPV has been studied in other epithelial contexts, and surveying that breadth helps situate the gut findings without overstating them.
Airway and epithelial inflammation models
The Land study was conducted in human bronchial epithelial cells, where KPV inhibited NF-κB and the inflammatory mediators MMP-9, IL-8, and eotaxin — demonstrating that the NF-κB-directed mechanism is not confined to intestinal tissue.[8] The broader alpha-MSH immunology literature likewise frames KPV’s effects on NF-κB, adhesion molecules, and cytokines as a general anti-inflammatory signaling motif rather than a tissue-specific one.[3]
Antimicrobial activity in vitro
Beyond inflammation, Cutuli and colleagues reported that both alpha-MSH and its C-terminal KPV tripeptide showed antimicrobial activity in vitro against Staphylococcus aureus and Candida albicans.[1] This breadth illustrates the range of research questions the tripeptide has been used to probe; it is not a basis for any application claim. One caveat for accurate citation: the later Songok work found that certain acetylated and glycoalkylated KPV analogs did not retain antimicrobial activity in the assays tested, so antimicrobial findings are specific to the forms studied and should not be generalized across all KPV derivatives.[12]
Research Handling, Stability, and Dosing Context
Apex provides handling context for laboratory work only; nothing in this section constitutes a dosing recommendation for humans, and no human dosing protocol for KPV exists in the cited literature. The administration data are entirely from cell-culture and rodent studies.
Proteolytic lability and concentration ranges in the literature
KPV is a small, enzymatically labile tripeptide, and the literature explicitly notes its susceptibility to proteolytic degradation and rapid elimination.[12] In cell-based work, the active concentrations reported are low — the cornerstone intestinal study described effects in the nanomolar range — which is relevant when planning in-vitro exposure conditions.[7] Because the peptide degrades readily, freshly prepared solutions and minimized freeze-thaw cycling are standard precautions.
Reconstitution and storage guidance for laboratory use
As a lyophilized tripeptide, KPV is generally stored dry at −20°C, with reconstituted aliquots held at −80°C and freeze-thaw cycles kept to a minimum to preserve integrity. These are general peptide-handling conventions rather than compound-specific stability data, and the rapid-degradation literature underscores why they matter for a labile small peptide. For protocol detail, consult the Apex guides on how to reconstitute peptides and peptide storage. No murine schedule can be translated to a human protocol; species-specific pharmacokinetics and the absence of human safety data make such extrapolation scientifically unsupportable.
Quality and Identity Verification: COA, HPLC, and ESI-MS
For a peptide as small and as labile as KPV, knowing exactly what is in the vial is not a formality — it directly determines whether an experiment is interpretable. A three-residue sequence offers little room for ambiguity, but it also means that a single substitution, truncation, or degradation product can change the molecule being tested.
Why HPLC purity and ESI-MS identity matter for a labile tripeptide
Reversed-phase high-performance liquid chromatography (HPLC) quantifies purity by separating the intended peptide from synthesis byproducts and degradation species, while electrospray-ionization mass spectrometry (ESI-MS) confirms identity by matching the measured mass to the expected value — 342.43 g/mol for the C16H30N4O4 Lys-Pro-Val sequence. Given the documented proteolytic lability of KPV, mass-spectrometric confirmation that the intact tripeptide is present is particularly valuable. Background on these methods is available in the Apex primers on how to read a peptide certificate of analysis and HPLC testing for peptide purity.
Reproducibility in research depends on documented identity
A research-grade certificate of analysis reporting ≥99% HPLC purity together with ESI-MS identity confirmation gives researchers documented confidence that the molecule under study is the intended 342.43-Da Lys-Pro-Val sequence. That documentation is what supports reproducibility across experiments and laboratories; these specifications describe research material quality and do not imply any therapeutic standard.
Safety, Tolerability & Adverse-Event Observations (Research Context)
In published preclinical research, the studies that report KPV’s anti-inflammatory effects also report on how the animals tolerated administration. These are tolerability observations documented in animal-model experiments, not patient side-effects, clinical safety findings, or any indication of what a person should expect; no human safety data for KPV exist in the cited literature.
Tolerability in murine colitis and inflammation models
In published murine research, KPV was generally well tolerated at the doses studied. Kannengiesser and colleagues reported that across dextran-sodium-sulfate (DSS) and CD45RB-high transfer colitis models KPV not only reduced inflammation, weight loss, histologic infiltrate, and myeloperoxidase activity but rescued all of the MC1-receptor-nonfunctional mice from death during DSS colitis — a survival observation in animals, framed strictly as a research finding.[11] In the foundational Dalmasso work, orally administered KPV reduced DSS- and TNBS-induced colitis without the investigators reporting overt adverse effects at the nanomolar-range exposures used, consistent with a defined signaling interaction rather than a nonspecific high-dose effect.[7]
Why these observations are not a human safety profile
Targeted-delivery work in a mouse ulcerative-colitis model likewise described accelerated mucosal healing and downregulated TNF-alpha following KPV delivery, again as a documented model outcome rather than a tolerability claim for any species beyond the one studied.[9] None of these animal-model tolerability observations has been established in humans, and none should be read as evidence of safety, efficacy, or an absence of adverse events in any clinical context. KPV remains a research-grade chemical reagent for in-vitro and preclinical use only, and the documented proteolytic lability of the tripeptide is a handling consideration for experimental reproducibility, not a pharmacological safety parameter.[12] Researchers preparing the reagent should review the Apex guides on how to reconstitute peptides and peptide storage.
Sourcing Research-Grade KPV
For any KPV experiment, reproducibility depends on knowing exactly what is in the vial. Because KPV is a small, labile tripeptide whose sequence identity and purity directly affect experimental outcomes, research-grade material should be accompanied by analytical documentation rather than label claims alone.
HPLC purity and ESI-MS identity verification
Apex supplies KPV at ≥99% purity, verified by reversed-phase HPLC for purity and by electrospray-ionization mass spectrometry (ESI-MS) for identity, confirming the expected mass near 342.43 g/mol against the C16H30N4O4 formula and the Lys-Pro-Val sequence. Each lot is documented with a per-batch certificate of analysis available through the lab-verified COA archive; researchers should review the lot-specific COA rather than relying on a generic specification.
Research-use-only designation and adjacent reagents
KPV is sold strictly for in-vitro and preclinical laboratory research and is not for human or veterinary use. The Apex editorial standards and research library document how each guide is sourced and reviewed. Researchers assembling a tissue-repair and anti-inflammatory reagent panel often pair KPV with related compounds; adjacent guides such as BPC-157 and GHK-Cu situate it within the broader research context, and the items below are available as research reagents.
KPV peptide and Adjacent Research Reagents
KPV
C-terminal alpha-MSH tripeptide (Lys-Pro-Val) anti-inflammatory research reagent; supplied at ≥99% purity verified by HPLC and mass spectrometry.
View ProductBPC-157
Gastric pentadecapeptide; widely studied cytoprotection/gut-repair research comparator.
View ProductGHK-Cu
Copper tripeptide; ECM-remodeling and anti-inflammatory tissue-research reagent.
View ProductFrequently Asked Questions
What is the KPV peptide?
KPV is a tripeptide composed of lysine, proline, and valine (Lys-Pro-Val), corresponding to residues 11 to 13 at the C-terminus of alpha-melanocyte-stimulating hormone (alpha-MSH). It has a molecular weight of approximately 342.43 g/mol (formula C16H30N4O4, CAS 67727-97-3). In the research literature it is studied as an anti-inflammatory melanocortin-derived peptide. Apex Laboratory supplies KPV as a research-grade chemical reagent for in-vitro and preclinical research only.
How does KPV reduce inflammation in research models?
Published preclinical studies report that KPV modulates inflammatory signaling rather than acting as a classical receptor agonist. In intestinal epithelial and immune cell models, nanomolar KPV has been shown to inhibit NF-κB and MAP-kinase pathways and reduce pro-inflammatory cytokine output (Dalmasso 2008). Airway-epithelial work describes a receptor-independent mechanism in which KPV suppresses p65RelA nuclear import via the importin-alpha pathway (Land 2012). These are cell-culture and rodent findings and have not been established in humans.
What is the half-life and stability of KPV in research conditions?
KPV is a small, enzymatically labile tripeptide. The published literature notes that peptides including KPV are susceptible to proteolytic degradation and rapid elimination, which is why investigators developed structurally modified, glycoalkylated analogs with improved stability toward proteolytic enzymes (Songok 2018). No defined human half-life exists, since all KPV pharmacokinetic context comes from cell-culture and rodent work. For in-vitro use this lability is why freshly prepared solutions and minimized freeze-thaw cycling are standard handling precautions.
How is KPV reconstituted and stored for laboratory research?
As a lyophilized tripeptide, KPV is generally reconstituted in a suitable research-grade solvent, stored dry at minus 20 degrees Celsius, with reconstituted aliquots held at minus 80 degrees Celsius and freeze-thaw cycles minimized to preserve integrity. These are general peptide-handling conventions rather than compound-specific stability data, and they matter because KPV degrades readily. Apex provides protocol detail in its how-to-reconstitute-peptides and peptide-storage guides. None of this constitutes a human dosing or administration instruction.
What doses of KPV have been used in published studies?
Doses are reported only as facts of published animal and cell experiments, never as recommendations. Cell-based intestinal studies described anti-inflammatory effects in the nanomolar concentration range (Dalmasso 2008), and murine colitis studies administered KPV orally or via targeted nanoparticle delivery to colonic tissue (Kannengiesser 2008; Xiao 2017). No human dosing protocol for KPV exists in the literature, and murine schedules cannot be translated to humans because species-specific pharmacokinetics and the absence of human safety data make such extrapolation unsupportable.
What adverse events or tolerability has KPV research reported?
In published murine research, KPV was generally well tolerated at the doses studied. Colitis-model work reported reduced inflammation, weight loss, and histologic injury, and one study rescued all MC1-receptor-nonfunctional mice from death during DSS colitis (Kannengiesser 2008); targeted-delivery work reported accelerated mucosal healing (Xiao 2017). These are animal-model tolerability observations framed as research findings only. No human safety data exist, and none of this should be read as patient side-effect information or a safety claim.
How is KPV different from full-length alpha-MSH and other melanocortin agonists?
Comparative pharmacology studies report that KPV behaves differently from core or full-length melanocortin peptides: it does not increase cAMP, its activity is not blocked by the MC3/4-receptor antagonist SHU9119, and it remains active in mice with a nonfunctional MC1 receptor (Getting 2003). Reviews note KPV lacks the sequence motif needed to bind known melanocortin receptors yet retains anti-inflammatory activity without the pigmentary action of alpha-MSH (Brzoska 2010). Researchers interpret this to mean KPV likely acts largely independently of classical melanocortin receptors.
Why do HPLC and ESI-MS verification matter for KPV?
KPV is a small, enzymatically labile tripeptide, and the published literature notes its susceptibility to proteolytic degradation (Songok 2018). For reproducible in-vitro work, confirming identity and purity matters: a research-grade certificate of analysis reporting greater-than-or-equal-to 99% HPLC purity together with ESI mass-spectrometry identity confirmation gives researchers documented confidence that the 342.43-Da Lys-Pro-Val sequence is what is being tested.
Continue Your Research
Researchers building broader context across the Apex Research Library may find the following references useful:
- Tissue Repair Research Peptides — the cluster hub situating KPV among anti-inflammatory and tissue-repair reagents
- BPC-157 Research Guide — the gastric pentadecapeptide studied as a cytoprotection and gut-repair comparator
- GHK-Cu Research Guide — the copper tripeptide studied for ECM remodeling and anti-inflammatory signaling
- BPC-157 vs GHK-Cu — two tissue-repair reagents compared across mechanism and study design
- How to Reconstitute Peptides — general protocol for preparing labile lyophilized peptides like KPV for in-vitro work
- Peptide Storage Guide — storage and freeze-thaw handling that preserve a degradation-prone tripeptide
- How to Read a Peptide Certificate of Analysis — interpreting HPLC purity and ESI-MS identity data on a lot-specific COA
- HPLC Testing for Peptide Purity — how reversed-phase HPLC quantifies purity for small peptides such as KPV
Research Use Disclaimer
All KPV products and the information in this guide are intended strictly for in-vitro and preclinical laboratory research. KPV is a research-grade chemical reagent and is not a drug, dietary supplement, or therapeutic product. It is not approved by the FDA, EMA, or any other regulatory authority, and it has no approved indication anywhere. It is not for human or veterinary consumption, diagnosis, treatment, or any clinical use. The mechanistic, anti-inflammatory, gut-model, and antimicrobial findings summarized here derive from cell-culture and animal-model studies and are presented for research context only; they do not constitute therapeutic, efficacy, or safety claims. Researchers are responsible for compliance with all applicable institutional, local, and national regulations governing the acquisition, handling, and use of research chemicals.
