
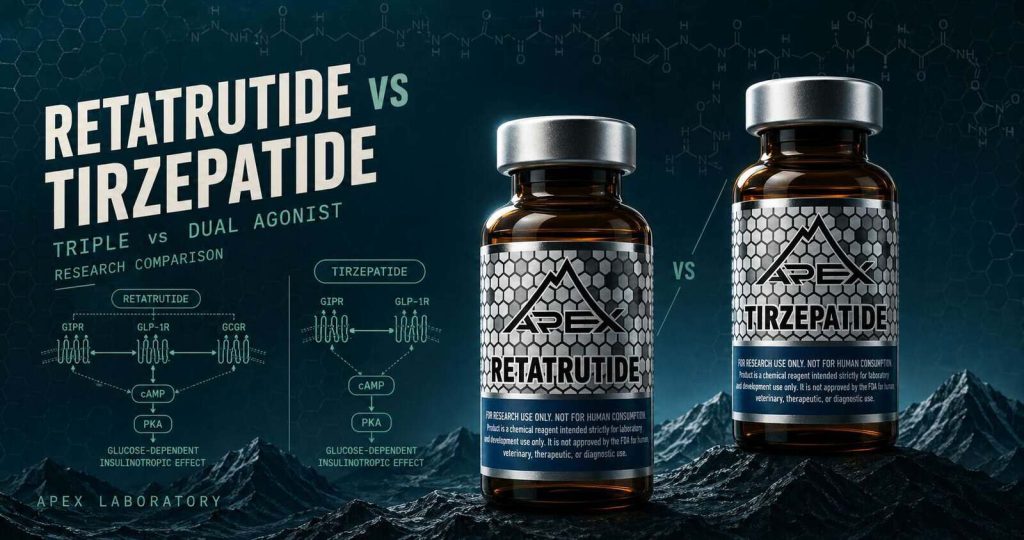
Retatrutide and Tirzepatide are GLP-1-family research peptides separated by a defining regulatory asymmetry — Tirzepatide is FDA-approved as Mounjaro and Zepbound, Retatrutide remains research-only. Tirzepatide is a dual GIP/GLP-1 receptor agonist; Retatrutide is a triple GIP/GLP-1/glucagon agonist with broader receptor engagement. Trial evidence comes from SURPASS/SURMOUNT for Tirzepatide and the TRIUMPH program for Retatrutide.
Tirzepatide is the active ingredient in two FDA-approved pharmaceuticals from Eli Lilly — Mounjaro, approved May 13, 2022 for type 2 diabetes, and Zepbound, approved November 8, 2023 for chronic weight management. Retatrutide (LY3437943), also from Lilly, has no FDA, EMA, or other regulatory approval anywhere in the world. The TRIUMPH clinical program remains pre-NDA, with Phase 2 dose-finding data published in 2023 and Phase 3 trials ongoing as of 2026. The two compounds sit at fundamentally different points along both axes that define this comparison. One axis is the structural-pharmacology progression from single-agonist (Semaglutide) to dual-agonist (Tirzepatide) to triple-agonist (Retatrutide). The other is the clinical-development pipeline from registrational Phase 3 SURPASS and SURMOUNT data to pre-NDA Phase 2 TRIUMPH readouts. Comparing them is comparing across an approval-status divide, not within a single class.
This guide provides an evidence-based head-to-head of retatrutide vs tirzepatide for researchers — covering regulatory positions, the structural-pharmacology progression from single- to dual- to triple-receptor agonism, the dual-agonist (GIP/GLP-1) versus triple-agonist (GIP/GLP-1/glucagon) mechanism contrast, the SURPASS and SURMOUNT Phase 3 versus TRIUMPH Phase 2 trial-program contrast under explicit phase-attribution discipline, and the Apex catalog framing for both compounds as research-grade material.
Retatrutide vs Tirzepatide at a Glance
- Tirzepatide is the active ingredient in Mounjaro (FDA-approved May 13, 2022 for type 2 diabetes) and Zepbound (FDA-approved November 8, 2023 for chronic weight management); Retatrutide (LY3437943) has no FDA, EMA, or other regulatory approval and is research-only globally with the Lilly TRIUMPH program pre-NDA
- The two compounds sit along a three-stage structural-pharmacology progression: single-agonist GLP-1R (Semaglutide reference class) → dual GIP/GLP-1 receptor engagement (Tirzepatide) → triple GIP/GLP-1/glucagon receptor engagement (Retatrutide)
- Both are 39-amino-acid synthetic peptides designed for once-weekly subcutaneous administration; Tirzepatide carries an approximately 5-day plasma half-life, Retatrutide approximately 6 days, and the third receptor — glucagon — recruits a hepatic energy-expenditure pathway absent from the dual-agonist profile
- Tirzepatide’s evidence base is the SURPASS T2D and SURMOUNT obesity Phase 3 registrational trial programs that supported the Mounjaro and Zepbound approvals; Retatrutide’s evidence base is the Phase 2 dose-finding TRIUMPH program, and the two trial generations are not directly comparable as efficacy claims
- Apex Laboratory’s research-grade Tirzepatide is a chemical research reagent distinct from the approved Mounjaro and Zepbound formulations; Apex’s research-grade Retatrutide is the only formulation that exists anywhere — both supplied at ≥99% purity for in-vitro and preclinical research
Regulatory Positions: The Defining Asymmetry
Regulatorily, Retatrutide and Tirzepatide occupy fundamentally different positions in the pharmaceutical pipeline. Tirzepatide is a marketed pharmaceutical with two distinct FDA approvals; Retatrutide has none.
Tirzepatide: Mounjaro (May 13, 2022) and Zepbound (November 8, 2023)
Tirzepatide is the active ingredient in two FDA-approved formulations marketed by Eli Lilly under distinct trade names for distinct indications. The FDA approved Mounjaro on May 13, 2022 as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes. The FDA approved Zepbound on November 8, 2023 for chronic weight management in adults with obesity (BMI ≥30) or overweight (BMI ≥27) with at least one weight-related comorbidity. Both formulations are pre-filled subcutaneous pens at 2.5, 5, 7.5, 10, 12.5, and 15 mg dose strengths. The two approvals are separate events under separate trade names for separate indications; the dates and indications must not be conflated.
Retatrutide: Pre-NDA, TRIUMPH Program, Research-Only Globally
Retatrutide — Eli Lilly’s research code LY3437943 — has no FDA approval, no EMA approval, and no regulatory approval in any other jurisdiction worldwide. The TRIUMPH clinical program is pre-NDA: Lilly published Phase 2 dose-finding data in obesity and type 2 diabetes in 2023 in NEJM and Lancet, and Phase 3 trials are ongoing as of 2026. The compound is an investigational triple-receptor agonist in active Phase 2/Phase 3 clinical development; no regulatory inevitability is implied or asserted, and no comparative pharmaceutical-brand framing applies to the research-grade reagent.
Why This Asymmetry Matters for the Comparison
Comparing across an approval-status divide is fundamentally different from comparing within a class. Trial-phase evidence is therefore not directly comparable as efficacy claims — the SURPASS and SURMOUNT Phase 3 trials are registrational evidence supporting marketed-pharmaceutical approvals, while the TRIUMPH Phase 2 trials are dose-finding evidence informing pre-NDA development decisions. Both compounds end up in the Apex catalog as research-grade material for different reasons, articulated under the Cerebrolysin-precedent regulatory framing pattern below.
Structural-Pharmacology Progression: Single → Dual → Triple Agonist
For broader GLP-1 context, see GLP-1 / metabolic research peptides and GLP-1 agonists compared.
Viewed structurally, the GLP-1 and multi-agonist research program advances along a clear progression: single-agonist GLP-1R engagement (Semaglutide, Liraglutide, Dulaglutide as the reference class) → dual GIP/GLP-1 receptor engagement (Tirzepatide) → triple GIP/GLP-1/glucagon receptor engagement (Retatrutide). Each receptor addition recruits an additional metabolic signaling pathway.
Single-Agonist Reference Class: Semaglutide and Earlier GLP-1Rs
Semaglutide, Liraglutide, and Dulaglutide constitute the single-agonist reference class — each built on a modified GLP-1 backbone, engaging GLP-1R alone. The canonical physiology of GLP-1 receptor signaling — glucose-dependent insulin secretion, glucagon suppression, gastric-emptying delay, and central appetite signaling — was synthesized by 1 Holst (2007) in Physiological Reviews and extended in the multi-author 2 Müller et al. (2019) review in Molecular Metabolism (co-authored by Drucker, Habener, Holst, Nauck, and DiMarchi). The within-class Semaglutide-vs-Tirzepatide SURPASS-2 head-to-head covers the single-vs-dual-agonist clinical contrast.
Dual-Agonist Step: Tirzepatide Adds GIP
Tirzepatide’s structural innovation is the engagement of GIP and GLP-1 receptors on a single 39-amino-acid synthetic peptide — built on a modified GIP backbone (not a modified GLP-1 backbone) with a C20 fatty-diacid moiety acylated to a lysine residue for albumin binding. Tirzepatide was first characterized by 3 Coskun and colleagues at Eli Lilly in Molecular Metabolism (2018), in a discovery-to-clinical-proof-of-concept paper covering molecular pharmacology, dual receptor engagement, preclinical efficacy, and Phase 1 pharmacokinetics. Adding the GIP receptor recruits glucose-dependent insulin secretion alongside modulation of glucagon secretion and adipose-tissue lipid handling absent from single-agonist GLP-1 engagement.
Triple-Agonist Step: Retatrutide Adds Glucagon
Retatrutide extends the dual-agonist class by engaging the glucagon receptor as a third target alongside GIPR and GLP-1R. 4 Coskun et al. (2022) characterized LY3437943 in Cell Metabolism under a journal-template structurally identical to the 2018 Tirzepatide paper — same first author, same Eli Lilly group, same “From discovery to clinical proof of concept” framing, four years apart. 5 Drucker (2024) in the Journal of Clinical Investigation contextualizes this arc within the broader multi-agonist landscape, from 1987 GLP-1 cloning through the contemporary triple-agonist frontier. Full Retatrutide depth sits at the Retatrutide research guide, with the broader six-family taxonomy in the forthcoming GLP-1 / Metabolic Research Peptides pillar.
Receptor Engagement and Mechanism Contrast
Critically, published pharmacological characterization has revealed that the dual- and triple-agonist mechanisms differ not only in the number of receptors engaged but in how each receptor is engaged. GIPR, GLP-1R, and GCGR (glucagon receptor) are all class B G-protein-coupled receptors; characterizing how each compound signals through them is the work that distinguishes the dual- from the triple-agonist class.
Tirzepatide: Dual GIP/GLP-1 with Biased Agonism
Published in Molecular Metabolism, 3 Coskun et al. (2018) documented Tirzepatide’s 39-amino-acid structure with C20 fatty-diacid acylation and an approximately 5-day plasma half-life (~120 hours). The most pharmacologically distinctive Tirzepatide finding sits at GLP-1R: research documented by 6 Willard et al. (2020) in JCI Insight characterizes Tirzepatide as “an imbalanced and biased dual GIP and GLP-1 receptor agonist” — engagement of GIPR and GLP-1R is imbalanced across the two targets, and at GLP-1R Tirzepatide preferentially recruits Gαs-protein over β-arrestin (a biased agonism signature distinct from the balanced single-receptor engagement of Semaglutide). Trial protocols administered Tirzepatide at 5, 10, and 15 mg weekly subcutaneous across the SURPASS and SURMOUNT programs.
Retatrutide: Triple GIP/GLP-1/Glucagon (LY3437943)
Retatrutide is also a 39-amino-acid synthetic peptide — same overall length as Tirzepatide, distinct receptor-engagement profile. Published in Cell Metabolism, 4 Coskun et al. (2022) characterized LY3437943 as engaging GIPR, GLP-1R, and the glucagon receptor on a single molecule. Retatrutide’s plasma half-life is approximately 6 days (~140–160 hours, dose-dependent), supporting once-weekly subcutaneous administration. The LY3437943 vs tirzepatide molecular-identity contrast is the addition of a third receptor target, not a different sequence length or injection cadence. Trial protocols administered Retatrutide at 1, 2, 4, 8, and 12 mg weekly subcutaneous in the TRIUMPH Phase 2 obesity trial.
What the Third Receptor Adds: Glucagon-Receptor Hepatic Energy Expenditure
GIPR engagement contributes glucose-dependent insulin secretion alongside glucagon-secretion and lipolysis modulation; GLP-1R engagement contributes insulin secretion, glucagon suppression, gastric-emptying delay, and appetite signaling. The proposed mechanistic rationale for the triple-agonist design rests on the third receptor: the glucagon receptor recruits hepatic glycogenolysis, gluconeogenesis, and energy expenditure / lipid oxidation pathways absent from dual-agonist engagement. 5 Drucker (2024) characterizes this third axis as the metabolic distinguisher between the dual- and triple-agonist generations.
Trial Program Contrast: SURPASS/SURMOUNT vs TRIUMPH
The clinical-development asymmetry between Retatrutide and Tirzepatide is as load-bearing as the structural one. Tirzepatide’s evidence base is the Phase 3 registrational SURPASS T2D and SURMOUNT obesity programs that supported the Mounjaro and Zepbound FDA approvals. Retatrutide’s evidence base is the Phase 2 dose-finding TRIUMPH program — pre-NDA, with Phase 3 trials ongoing.
Tirzepatide Phase 3: SURPASS T2D and SURMOUNT Obesity
The full SURPASS and SURMOUNT enumeration sits in a forthcoming standalone Tirzepatide research guide; two anchor trials suffice here. SURPASS-2 — Phase 3 head-to-head against Semaglutide published in NEJM by 7 Frías et al. (2021) — randomized 1,879 patients with T2D over 40 weeks, reporting HbA1c reductions of −2.01, −2.24, and −2.30 percentage points (5/10/15 mg) versus −1.86 for Semaglutide 1 mg. SURMOUNT-1 — the foundational obesity trial published in NEJM by 8 Jastreboff et al. (2022) — randomized 2,539 adults with obesity over 72 weeks, reporting body weight reductions of −15.0%, −19.5%, and −20.9% (5/10/15 mg) versus −3.1% placebo. Per-protocol analyses reported approximately 22.5% body weight reduction at the highest tolerated dose; the −15.0/−19.5/−20.9% figures are the primary trial-attributed numbers. These trials are Phase 3 registrational — the foundation for Mounjaro May 13, 2022 and Zepbound November 8, 2023 FDA approvals.
Retatrutide Phase 2: TRIUMPH Obesity and T2D Readouts
The TRIUMPH Phase 2 obesity readout — 9 Jastreboff et al. (2023) in NEJM — randomized 338 adults with obesity over 48 weeks, reporting body weight reductions of −8.7%, −17.1%, −22.8%, and −24.2% (1/4/8/12 mg) versus −2.1% placebo. The TRIUMPH Phase 2 T2D readout — 10 Rosenstock et al. (2023) in Lancet — studied 281 T2D participants over 36 weeks against placebo with a dulaglutide 1.5 mg active comparator (used for safety and PK assay validation, not as a primary head-to-head efficacy comparator), reporting up to approximately 17% body weight reduction at the 8 and 12 mg doses and HbA1c <6.5% in up to 82% of participants. These are Phase 2 dose-finding readouts — pre-NDA, research-only globally. Full Retatrutide Phase 2 depth sits at the Retatrutide research guide.
Why Phase 3 vs Phase 2 Readouts Are Not Directly Comparable
In the SURMOUNT-1 Phase 3 obesity trial (Jastreboff et al., 2022, NEJM), Tirzepatide 15 mg produced body weight reductions of −20.9% at 72 weeks in 2,539 adults with obesity. In the TRIUMPH Phase 2 obesity trial (Jastreboff et al., 2023, NEJM), Retatrutide 12 mg produced reductions of −24.2% at 48 weeks in 338 adults. These trials are at different regulatory-readiness phases (Phase 3 registrational vs Phase 2 dose-finding), with different sample sizes, durations, patient populations, and control-arm designs, and are not directly comparable as efficacy claims. The same first author (Jastreboff AM) appears on both trials. That continuity makes the discipline-boundary qualifier more important, not less. The retatrutide vs tirzepatide weight loss comparison that dominates competitor SERPs flattens these phase-distinct readouts into a winner-loser framing. The underlying trial designs do not support that framing.
Retatrutide vs Tirzepatide
| Attribute | Retatrutide | Tirzepatide |
|---|---|---|
| Mechanism | Triple receptor agonist (GIP/GLP-1/glucagon); 39-amino-acid synthetic peptide (Coskun 2022) | Dual receptor agonist (GIP/GLP-1); 39-amino-acid synthetic peptide on modified GIP backbone with C20 fatty-diacid acylation (Coskun 2018) |
| Receptor engagement | GIPR + GLP-1R + GCGR; third-receptor engagement recruits hepatic energy-expenditure pathway | GIPR + GLP-1R; biased agonism at GLP-1R (Gαs-skewed; Willard 2020); imbalanced GIPR vs GLP-1R engagement |
| Sequence length | 39 amino acids | 39 amino acids |
| Half-life | Approximately 6 days (~140–160 hours, dose-dependent) | Approximately 5 days (~120 hours) |
| Dosing frequency (trial protocols) | Once-weekly subcutaneous; trial-protocol doses 1 / 2 / 4 / 8 / 12 mg (TRIUMPH Phase 2) | Once-weekly subcutaneous; trial-protocol doses 5 / 10 / 15 mg (SURPASS / SURMOUNT Phase 3) |
| Trial program phase | Phase 2 dose-finding (TRIUMPH program); Phase 3 trials ongoing | Phase 3 registrational (SURPASS T2D 1–5; SURMOUNT obesity 1–4) |
| Regulatory status | No FDA, EMA, or other regulatory approval; pre-NDA; research-only globally | Active ingredient in Mounjaro (FDA-approved May 13, 2022 — type 2 diabetes) and Zepbound (FDA-approved November 8, 2023 — chronic weight management) |
| Apex catalog status | Available as research-grade chemical reagent; the only formulation that exists anywhere | Available as research-grade chemical reagent; distinct from approved Mounjaro and Zepbound pharmaceutical formulations |
| Lead developer | Eli Lilly and Company | Eli Lilly and Company |
| First clinical report year | 2022 (Coskun et al., Cell Metabolism; LY3437943 discovery + Phase 1 PoC) | 2018 (Coskun et al., Molecular Metabolism; LY3298176 discovery + Phase 1 PoC) |
Apex Catalog: Both Research-Grade, for Different Reasons
Apex Laboratory’s catalog includes both compounds as research-grade material — but the two end up in the same catalog tier for different reasons. Apex’s research-grade Tirzepatide is a chemical research reagent distinct from the FDA-approved Mounjaro (May 13, 2022, type 2 diabetes) and Zepbound (November 8, 2023, chronic weight management) pharmaceutical formulations, supplied at ≥99% purity verified by HPLC and mass spectrometry under the editorial standards and lab-verified COA archive for in-vitro and preclinical research only. Apex’s research-grade Retatrutide, by contrast, is the only formulation of LY3437943 that exists anywhere — no approved pharmaceutical formulation exists, because the TRIUMPH program is pre-NDA. The retatrutide vs tirzepatide catalog framing routes through the Apex research library under the GLP-1 / Metabolic Research category.
Research-Grade Compounds for This Comparison
Retatrutide
Apex Laboratory Retatrutide (LY3437943) is supplied as a research-grade chemical reagent at ≥99% purity, verified by HPLC and mass spectrometry on every batch and documented in the lab-verified COA archive. Triple GIP/GLP-1/glucagon receptor agonist; the only formulation that exists anywhere. For in-vitro and preclinical research only — not for human consumption.
View Product →Tirzepatide
Apex Laboratory Tirzepatide is supplied as a research-grade chemical reagent at ≥99% purity, verified by HPLC and mass spectrometry on every batch. Dual GIP/GLP-1 receptor agonist; research-grade material distinct from the FDA-approved Mounjaro and Zepbound pharmaceutical formulations. For in-vitro and preclinical research only — not for human consumption.
View Product →Frequently Asked Questions
What is the difference between retatrutide and tirzepatide?
Retatrutide (LY3437943) is a triple GIP/GLP-1/glucagon receptor agonist; Tirzepatide (LY3298176) is a dual GIP/GLP-1 receptor agonist. Both are 39-amino-acid synthetic peptides developed by Eli Lilly for once-weekly subcutaneous administration. Tirzepatide is FDA-approved as Mounjaro and Zepbound, while Retatrutide is research-only globally with the TRIUMPH program pre-NDA. The retatrutide tirzepatide comparison is across an approval-status divide.
Is retatrutide FDA-approved?
No. Retatrutide has no FDA, EMA, or other regulatory approval anywhere in the world. Eli Lilly’s TRIUMPH clinical program remains pre-NDA, with Phase 2 dose-finding data published in 2023 in NEJM and Lancet and Phase 3 trials ongoing as of 2026. Retatrutide is classified as a research compound globally; Apex Laboratory’s research-grade Retatrutide is the only formulation that exists anywhere.
What does triple agonist mean compared to dual agonist?
A triple agonist is a single molecule engaging three receptors — for Retatrutide, GIPR plus GLP-1R plus the glucagon receptor. A dual agonist engages two — for Tirzepatide, GIPR plus GLP-1R. Single-agonist GLP-1 compounds (Semaglutide, Liraglutide, Dulaglutide) engage GLP-1R alone. The third receptor in Retatrutide recruits hepatic energy-expenditure signaling absent from dual-agonist engagement.
How do TRIUMPH and SURPASS trials compare?
SURPASS (Tirzepatide T2D) and SURMOUNT (Tirzepatide obesity) are the Phase 3 registrational programs that supported the Mounjaro and Zepbound FDA approvals. TRIUMPH (Retatrutide) is the Phase 2 dose-finding program — Jastreboff 2023 NEJM obesity readout and Rosenstock 2023 Lancet T2D readout — and remains pre-NDA. Phase 3 registrational and Phase 2 dose-finding readouts are at different regulatory-readiness phases and not directly comparable as efficacy claims.
What weight-loss data has been reported for retatrutide compared to tirzepatide?
In the SURMOUNT-1 Phase 3 obesity trial (Jastreboff et al., 2022, NEJM), Tirzepatide 15 mg produced body weight reductions of −20.9% at 72 weeks in 2,539 adults. In the TRIUMPH Phase 2 obesity trial (Jastreboff et al., 2023, NEJM), Retatrutide 12 mg produced reductions of −24.2% at 48 weeks in 338 adults. These trials are at different regulatory-readiness phases with different durations and populations, and not directly comparable as efficacy claims.
What are the half-lives and dosing schedules for retatrutide and tirzepatide?
Retatrutide carries an approximately 6-day plasma half-life (~140–160 hours, dose-dependent); TRIUMPH Phase 2 trial protocols administered once-weekly subcutaneous doses of 1, 2, 4, 8, and 12 mg. Tirzepatide carries an approximately 5-day half-life (~120 hours); SURPASS and SURMOUNT Phase 3 trial protocols administered 5, 10, and 15 mg weekly subcutaneous. Trial-protocol dose ranges are descriptive trial-attribution facts, not consumption guidance.
Continue Your Research
Researchers building broader retatrutide vs tirzepatide context across the Apex library may find the following references useful, alongside the forthcoming GLP-1 / Metabolic Research Peptides pillar:
- Standalone Retatrutide research guide — full Phase 2 deep-dive on the TRIUMPH program and triple-agonist mechanism
- Semaglutide-vs-Tirzepatide SURPASS-2 head-to-head comparison — single-agonist vs dual-agonist clinical-data contrast
- Cerebrolysin research guide — parallel Cerebrolysin-precedent regulatory framing example
- Tissue repair research peptide pillar — lateral pillar covering BPC-157, TB-500, and the tissue-repair family
- Nootropic and CNS research peptide pillar — lateral pillar covering Selank, Semax, and the broader CNS research-peptide landscape
- Tirzepatide Research Guide
- Selank Research Guide
- BPC-157 Research Guide
- TB-500 (Thymosin Beta-4) Research Guide
Research Use Disclaimer
This article is provided for educational and research reference purposes only. Retatrutide, Tirzepatide, and all products sold by Apex Laboratory are intended exclusively for in-vitro laboratory research use and are not for human consumption. Researchers should consult the primary peer-reviewed literature for SURPASS, SURMOUNT, and TRIUMPH trial protocols and findings.
