
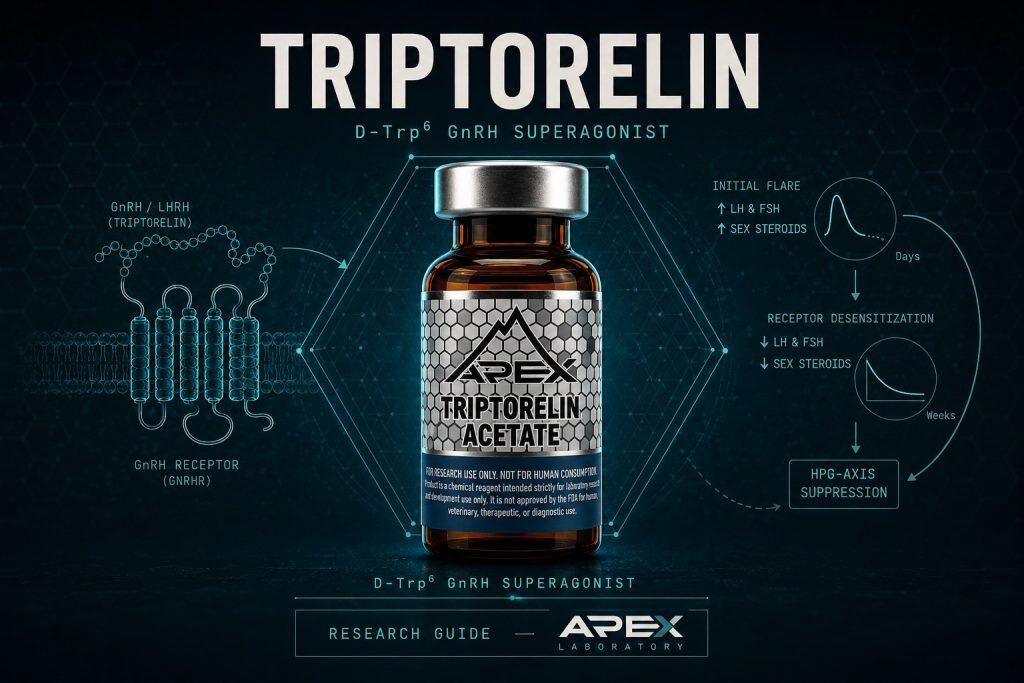
Triptorelin is a synthetic decapeptide gonadotropin-releasing hormone (GnRH/LHRH) receptor superagonist, structurally native GnRH with D-tryptophan substituted for glycine at position 6 (D-Trp6-LHRH). Continuous, non-pulsatile receptor stimulation first produces a brief agonist flare, then desensitizes and downregulates the pituitary GnRH receptor, profoundly suppressing luteinizing hormone, follicle-stimulating hormone, and downstream sex steroids. Apex Laboratory supplies triptorelin as a research-grade chemical reagent for in-vitro and preclinical research, distinct from the Trelstar and Triptodur pharmaceutical formulations.
Triptorelin presents a puzzle that trips up newcomers to neuroendocrine pharmacology: it is an agonist of the gonadotropin-releasing hormone (GnRH) receptor, yet its defining and most-studied effect is the near-complete suppression of the gonadotropins it should, in principle, release. A drug that activates a receptor in order to silence the downstream signal sounds like a contradiction. It is not. The apparent paradox dissolves once the timing of receptor occupancy is taken into account, and that distinction — pulsatile versus continuous stimulation — is precisely why triptorelin has become a durable tool for interrogating the hypothalamic-pituitary-gonadal (HPG) axis.[1]
This guide profiles triptorelin as a research-grade chemical reagent: its decapeptide structure and the single D-tryptophan-6 substitution that defines it, the superagonist mechanism that converts activation into suppression, its depot pharmacokinetics, and the HPG-axis research contexts in which it appears. Throughout, every pharmacological observation is framed as research-context evidence drawn from the published literature; nothing here is a therapeutic claim, and the same molecule’s regulatory status as an approved pharmaceutical is addressed separately in its own section. For broader context on this category, see the specialty research peptides hub.
Triptorelin at a Glance
- Triptorelin is a synthetic 10-residue GnRH/LHRH superagonist with the sequence pGlu-His-Trp-Ser-Tyr-D-Trp-Leu-Arg-Pro-Gly-NH₂ (CAS 57773-63-4, MW ≈1311.45 g/mol).
- A single glycine-6 → D-tryptophan-6 substitution confers enzymatic-degradation resistance and higher receptor affinity, producing the superagonist profile and an extended half-life versus native GnRH.
- The apparent paradox — an agonist that suppresses — resolves through continuous receptor occupancy: a transient flare gives way to GnRH-receptor desensitization and downregulation.
- Net effect in the literature is profound suppression of luteinizing hormone, follicle-stimulating hormone, and downstream sex steroids, with reported recovery after discontinuation.
- Depot and sustained-release formulations described in the literature extend exposure to roughly one, three, or six months, maintaining castrate-range testosterone in prostate-cancer research models.
- Triptorelin is the active molecule in the FDA-approved formulations Trelstar and Triptodur; Apex supplies it only as a research-grade chemical reagent, not as a pharmaceutical and not for human consumption.
Triptorelin Acetate
What Is Triptorelin? Structure, Identity, and Research Context
Triptorelin is a synthetic decapeptide — a ten-amino-acid chain — that is, structurally, native gonadotropin-releasing hormone with one deliberate change. Where native GnRH (also called luteinizing-hormone-releasing hormone, LHRH) carries a glycine at position 6, triptorelin substitutes a D-tryptophan residue, giving the molecule its common research designations D-Trp₆-LHRH and D-Trp₆-GnRH. The full sequence is pGlu-His-Trp-Ser-Tyr-D-Trp-Leu-Arg-Pro-Gly-NH₂, with a pyroglutamate at the N-terminus and a C-terminal amide.[2]
As a research reagent, triptorelin is typically supplied as a lyophilized acetate salt with a molecular formula of C64H82N18O13 and a free-base molecular weight near 1311.45 g/mol (CAS 57773-63-4). These values are corroborated by PubChem CID 25074470. One point worth flagging for catalog accuracy: the free-base CAS used for the reagent differs from the pamoate (embonate) salt employed in the long-acting pharmaceutical depots, so the two should not be conflated. Researchers verifying identity against a certificate of analysis can review how to read a peptide COA for the relevant fields.
Why a decapeptide framing matters
Because triptorelin differs from native GnRH at only a single position, it is a near-isosteric probe of the GnRH receptor: it engages the same binding pocket and the same signal-transduction machinery, which makes it valuable for studying receptor behavior under exposure conditions that endogenous GnRH never sustains. That structural near-identity, paired with a pharmacology that is anything but identical, is the through-line of everything that follows. Apex supplies this molecule strictly as a chemical reagent for in-vitro and preclinical research, not as a pharmaceutical and not for human consumption.
The GnRH/LHRH Axis: The Physiology Triptorelin Is Used to Probe
To understand why triptorelin behaves the way it does, the underlying circuitry has to be in view. The hypothalamic-pituitary-gonadal axis begins in the hypothalamus, where specialized neurons release GnRH in discrete pulses rather than as a steady stream. Each pulse reaches the anterior pituitary and stimulates gonadotroph cells, which in turn secrete two gonadotropins — luteinizing hormone (LH) and follicle-stimulating hormone (FSH) — into the circulation. LH and FSH then act on the gonads to drive the production of sex steroids such as testosterone and estradiol, completing the axis.
The pulsatility is not incidental; it is the signal. Decades of endocrine research show that the gonadotroph is tuned to intermittent receptor stimulation. When GnRH arrives in pulses, the receptor resets between signals and gonadotropin output is sustained. When the same receptor is occupied continuously, the gonadotroph adapts in the opposite direction — the cellular machinery that links receptor activation to hormone secretion is progressively withdrawn.[3] This pulsatile-versus-continuous distinction is the hinge on which the entire triptorelin paradox turns, and it is what a long-acting superagonist exploits. Native GnRH itself is available as a research reagent for the contrasting pulsatile case; see the gonadorelin versus triptorelin GnRH guide for that comparison.
Superagonist Mechanism: Flare First, Then Desensitization and Downregulation
Here the paradox resolves. When triptorelin first occupies the GnRH receptor, it behaves exactly as an agonist should: it activates the receptor and triggers an acute, transient surge of LH, FSH, and downstream sex steroids. This is the well-documented flare phenomenon, the hallmark of a superagonist at treatment initiation.[1] Because triptorelin is long-acting and binds tightly, however, that occupancy does not subside between pulses the way native GnRH does. The receptor is engaged continuously.
GnRH receptor (Class A GPCR) → continuous agonist occupancy → desensitization (phosphorylation, beta-arrestin, internalization) → receptor downregulation → LH/FSH and sex-steroid suppression
Triptorelin binds the pituitary GnRH receptor and initially activates it, producing the transient flare. Under the sustained, non-pulsatile occupancy that its extended half-life enforces, the gonadotroph withdraws the signal in two stages: desensitization, via agonist-induced receptor phosphorylation, beta-arrestin association, and internalization, followed by downregulation of surface receptor number. Because mammalian GnRH receptors lack a C-terminal tail, post-receptor steps carry much of the desensitization, as detailed by McArdle and colleagues (1999). The net documented outcome is profound suppression of LH, FSH, and downstream sex steroids.
Under that continuous exposure, the gonadotroph adapts. The published mechanistic literature describes a two-stage withdrawal: first desensitization, in which the receptor becomes functionally uncoupled from its signaling cascade, and then downregulation, in which the number of available receptors at the cell surface falls.[1] Mechanistic work on the GnRH receptor at the G-protein-coupled-receptor (GPCR) level, led by McArdle and colleagues, attributes desensitization to agonist-induced receptor phosphorylation, beta-arrestin association, and internalization. A structural curiosity is relevant here: mammalian GnRH receptors lack the C-terminal cytoplasmic tail that most GPCRs use as a phosphorylation substrate, so post-receptor mechanisms — including downregulation of the inositol-trisphosphate receptor — carry much of the desensitization load.[4]
The net effect
After the initial flare passes, the documented result of sustained superagonist exposure is profound suppression of LH, FSH, and the sex steroids they govern. The mechanism is therefore not a simple on-switch but a desensitizing one: activation that the cell answers by removing the signal. It is worth a precise note — some pharmacology reviews argue that triptorelin does not induce total pituitary shutdown, since the gonadotropin alpha-subunit can remain GnRH-responsive even as the beta-subunits are suppressed.[2] The accurate framing is flare-then-suppression with differential subunit effects, not a claim of complete receptor silencing.
The D-Trp6 Substitution: Why One Residue Changes Everything
If triptorelin is native GnRH with a single swap, that swap is doing a great deal of work. Replacing the glycine at position 6 with a D-tryptophan — a tryptophan in the non-natural D stereochemistry — produces two coordinated effects that together define the superagonist.
The first is resistance to enzymatic degradation. Native GnRH is cleaved rapidly by endopeptidases, giving it a short biological lifetime. Position 6 sits at a key cleavage region, and introducing a D-amino acid there blunts enzymatic attack, extending the molecule’s half-life. The second effect is increased affinity for the LHRH receptor. The bulkier, conformationally constrained D-tryptophan favors a receptor-bound geometry, so the analog binds harder and activates more potently than the native peptide.[2] Pharmacokinetic reviews of GnRH agonists report half-disappearance times several-fold longer than native GnRH precisely because of this substitution strategy.[3]
Longer half-life plus higher affinity is exactly the recipe for continuous receptor occupancy — which, per the previous section, is what converts agonism into suppression. The D-Trp₆ substitution is thus not a minor structural footnote; it is the molecular cause of the entire pharmacological cascade. This is also a useful illustration of why precise identity verification matters for reagents: a single stereochemical detail at one position is the difference between native GnRH and a superagonist.
Differential Gonadotropin-Subunit Effects: LH-Beta vs the Alpha-Subunit
The phrase “gonadotropin suppression” is a simplification that the careful literature resists. LH and FSH are each heterodimers: they share a common alpha-subunit and are distinguished by their hormone-specific beta-subunits. Under continuous GnRH-agonist exposure, these subunits are not regulated uniformly.
Pharmacokinetic and pharmacodynamic reviews report that the beta-subunits — LH-beta in particular — are predominantly suppressed, while the shared alpha-subunit can remain responsive or even be relatively preserved.[2][3] Preclinical work in the broader GnRH-agonist class supports this differential pattern: long-term agonist exposure in rodent models predominantly suppresses the beta-immunoreactive gonadotroph populations while sparing the alpha-glycoprotein subunit. That class-level rodent evidence comes from studies using other GnRH agonists rather than triptorelin specifically, so it is cited here as mechanistic context for the differential-subunit phenomenon, not as a triptorelin finding.
The practical upshot for researchers designing experiments is that “suppression” should be specified at the subunit level. Measuring total LH may miss the more granular regulation occurring beneath it, and conflating beta-subunit suppression with complete axis silencing overstates the effect. Mechanistic studies of GnRH-analogue action in pituitary gonadotrophs, where triptorelin has been used directly as the agonist test article, reinforce that the response is steroid-milieu dependent and not a simple all-or-nothing switch.[5]
Depot and Sustained-Release Pharmacokinetics
Continuous receptor occupancy is the goal, and formulation chemistry is how the literature achieves it. Even in immediate-release form, triptorelin shows a striking route-dependence: pharmacokinetic reviews report that the effective half-life after subcutaneous administration is roughly an order of magnitude longer than after intravenous dosing, because the peptide releases progressively from the injection-site depot rather than clearing in a single bolus.[2]
Sustained-release depot formulations extend that principle deliberately. The literature describes microsphere and polymer-matrix depots engineered to release triptorelin over approximately one, three, or six months from a single administration. A three-month sustained-release study in advanced prostate adenocarcinoma documented the characteristic profile: an early plasma surge corresponding to the flare, followed by stable depot-level concentrations, with testosterone driven into the surgical-castration range by roughly day 22 and maintained through day 91.[6] A review of six-month GnRH-agonist depots reported that triptorelin pamoate 22.5 mg achieved chemical castration — serum testosterone at or below 50 ng/dL — in roughly 93–99% of subjects across the relevant pivotal trials.[7]
These depot characteristics are clinical-trial observations summarized for research context; they describe the pharmacokinetic behavior of the molecule, not an endorsement of any use. For researchers handling the lyophilized reagent, reconstitution and concentration choices materially affect exposure in vitro — see how to reconstitute peptides and the peptide storage guide for handling that preserves integrity.
Agonist vs Antagonist Pharmacology: A Comparative View
The cleanest way to understand triptorelin’s mechanism is to set it against its mechanistic opposite: the GnRH (LHRH) antagonist. Both classes ultimately reduce gonadotropin output, but they get there by routes that are almost mirror images, and the difference has concrete consequences for experimental design.
GnRH Superagonist (Triptorelin) vs GnRH Antagonist vs Native GnRH
| Property | Triptorelin (superagonist) | GnRH antagonist | Native GnRH (gonadorelin) |
|---|---|---|---|
| Receptor action | Activates receptor, then desensitizes it | Competitively blocks receptor without activating | Activates receptor in physiologic pulses |
| Initial flare | Yes — transient LH/FSH/sex-steroid surge | No — immediate suppression | No flare; pulse-dependent stimulation |
| Net axis effect | Profound LH/FSH and sex-steroid suppression (after flare) | Prompt LH/FSH suppression | Sustained gonadotropin secretion (pulsatile) |
| Structural basis | D-tryptophan-6 substitution in decapeptide | Multiple substitutions for competitive blockade | Unmodified pGlu…Gly-NH₂ decapeptide |
| Typical research framing | Desensitization / sustained-suppression models | Flare-free suppression models | Pulsatile-stimulation / control comparator |
A GnRH antagonist binds the receptor and blocks it competitively without activating it. The result is immediate suppression with no flare — gonadotropin levels fall promptly because the receptor is occupied but never switched on. A superagonist like triptorelin does the reverse: it switches the receptor on hard, producing the flare, and only achieves suppression after the gonadotroph desensitizes and downregulates in response to the sustained signal. Comparative reviews of LHRH agonist and antagonist development frame this distinction precisely — agonists work through initial stimulation followed by desensitization and receptor downregulation, whereas antagonists act by direct competitive blockade that preserves the resting receptor.[8]
For a researcher, the choice between the two is a choice about kinetics and confounds. If a transient gonadotropin surge would corrupt an experimental readout, the flare-free antagonist may be preferable; if the goal is to study the desensitization process itself, the superagonist is the relevant tool. The receptor signaling also differs by site — pituitary versus extrapituitary tumor cells engage distinct G-protein pathways — which is itself an active area of receptor-pharmacology research.[1]
Discovery and Lineage: The Schally LHRH-Analog Program
Triptorelin descends directly from the foundational work that established LHRH as a discrete hypothalamic hormone. The research program led by Andrew V. Schally characterized LHRH and, in the early 1970s, pursued structure-activity refinement of the native decapeptide — including the synthesis of D-Trp₆-LHRH by substituting D-tryptophan at position 6. That single substitution, as the preceding sections describe, produced the superagonist now known as triptorelin.[2]
Early human pharmacology co-authored by Schally’s group demonstrated the analog’s signature effect: daily administration of D-Trp₆-LHRH drove plasma testosterone and dihydrotestosterone to castrate values and suppressed acutely releasable LH, with the effect reversing after discontinuation. That 1981 work explicitly proposed the analog as a means of achieving reversible, pharmacologic gonadal suppression in endocrine-dependent disease.[9] The molecule was subsequently developed into the depot pharmaceutical formulations marketed internationally; the attribution to the originating research program is preserved throughout the literature, and the reversibility-on-discontinuation finding remains a defining pharmacological characteristic. Apex’s editorial approach to such lineage attribution is described in its editorial standards.
Research Applications Across the HPG Axis
Because triptorelin produces a deep, reversible, and well-characterized suppression of the HPG axis, it appears across several research contexts as an investigational tool. None of the following is a therapeutic recommendation; each is a research application documented in the published literature.
Androgen-suppression and prostate-cancer research models
The earliest and most extensively documented context is androgen suppression. From the 1981 Schally-group human study onward, triptorelin has been used to drive testosterone into the castrate range reversibly, and depot formulations have been studied for sustained androgen-deprivation in prostate-cancer models.[9][7]
Reproductive and ovarian-stimulation pituitary down-regulation
In reproductive research, depot triptorelin is used to achieve pituitary desensitization and down-regulation so that the endogenous LH surge can be controlled in ovarian-stimulation protocols. A randomized study of half-dose depot triptorelin in assisted-reproduction-technology stimulation documented effective pituitary suppression without a premature LH surge.[10]
Central precocious puberty research context
Pediatric pharmacokinetic and pharmacodynamic reviews describe depot GnRH agonists, including triptorelin, in the central-precocious-puberty research context, where the goal is to deeply suppress prematurely activated gonadotropin secretion.[3]
In-vitro gonadotroph cell-line models
At the bench, GnRH-receptor desensitization is studied directly in gonadotroph-derived cell lines such as the alphaT3-1 line, an in-vitro model in which receptor loss and impaired calcium mobilization can be characterized under controlled agonist exposure.[11] Upstream regulators of GnRH release are studied alongside it; researchers working on that layer of the axis may find the kisspeptin-10 research guide a useful companion.
Dosing, Handling, and Experimental-Design Considerations
Apex does not provide therapeutic dosing instructions, and nothing in this section should be read as one. What the literature does offer is a set of reported exposure parameters and general peptide-handling practices relevant to reproducible in-vitro and preclinical work.
The single most important design variable is exposure pattern. Because triptorelin’s suppressive effect depends on continuous receptor occupancy, an experiment that delivers the peptide in a pulsatile or intermittent fashion may produce a fundamentally different gonadotroph response than one delivering sustained exposure — the difference between stimulating and suppressing the axis can come down to the dosing schedule rather than the dose itself. This is the practical face of the pulsatile-versus-continuous principle established earlier.
For handling, the lyophilized acetate powder is stored desiccated at −20°C, protected from light and moisture; reconstituted aliquots are kept frozen and freeze-thaw cycles are minimized to preserve peptide integrity. These are general peptide-research practices rather than compound-specific stability data, and researchers should confirm specifics against the lot certificate of analysis. Detailed protocols are covered in how to reconstitute peptides and the peptide storage guide. Reported study exposures — the daily 100 microgram regimens of the early human pharmacology, or the milligram-scale depot loadings of the sustained-release literature — describe published protocols and are not handling recommendations for any other context.[9]
Quality, Identity, and the COA Trust Angle
Reproducible HPG-axis research depends on knowing exactly what is in the vial. A single-residue stereochemical feature defines triptorelin, and a contaminating diastereomer or a truncated sequence would not announce itself by appearance — only analytical verification distinguishes the correct molecule from a near-miss. That is why identity and purity documentation are not bureaucratic overhead but a precondition for trustworthy data.
Apex specifies research-grade triptorelin at ≥99% purity verified by reversed-phase HPLC, with molecular identity confirmed by electrospray-ionization mass spectrometry (ESI-MS) against the expected mass near 1311 Da. Each batch is accompanied by a lot-specific certificate of analysis, archived in the lab-verified COA archive; researchers should read the COA for the specific lot in hand rather than assume a catalog-level figure. Guidance on interpreting those documents is available in how to read a peptide COA and HPLC testing for peptide purity.
The ≥99% HPLC and ESI-MS specification is a product-quality statement, not a pharmacological finding — it speaks to the integrity of the reagent, not to any effect. Apex’s verification approach and editorial methodology are documented in its editorial standards.
Regulatory Framing: Research-Grade Reagent vs FDA-Approved Formulations
Triptorelin occupies two categorically distinct regulatory worlds, and conflating them is the most common error in writing about the molecule. The same triptorelin that Apex supplies as a research reagent is also the active ingredient in two FDA-approved pharmaceutical products.
Trelstar (triptorelin pamoate, an injectable depot suspension available in 3.75 mg, 11.25 mg, and 22.5 mg strengths) was originally approved under NDA 020715 on June 15, 2000, and is labeled for the treatment of advanced prostate cancer as a GnRH agonist for androgen-deprivation. Triptodur (triptorelin extended-release for injectable suspension, a 22.5 mg six-month depot) was approved under NDA 208956 on June 29, 2017, and is labeled for pediatric central precocious puberty in patients two years and older. These approvals, dates, and indications are drawn from the FDA Drugs@FDA record; note that current sponsors of record differ from the historical developers and marketers of the molecule, so historical attributions should be treated with appropriate caution.
The principle is the canonical one: same molecule (triptorelin); categorically distinct regulatory frameworks. Trelstar and Triptodur are pharmaceutical formulations manufactured under pharmaceutical controls for defined clinical indications. A research-grade reagent is a lyophilized chemical supplied for in-vitro and preclinical research only — it is not a pharmaceutical, not for human consumption, and not a therapeutic equivalent to any approved product. This distinction is the subject of a dedicated explainer; researchers should read research-grade vs pharmaceutical-grade peptides for the full treatment.
Safety, Tolerability & Adverse-Event Observations (Research Context)
In published clinical and preclinical research, the adverse-event and tolerability profile of triptorelin follows predictably from its pharmacology: it is the documented profile of a GnRH superagonist that first stimulates and then deeply suppresses the hypothalamic-pituitary-gonadal axis. The observations summarized here are research findings reported in named studies and pharmacology reviews; they are not patient guidance, not a description of what any individual should expect, and not claims of safety or efficacy. Nothing in this section describes therapeutic use.
The flare effect as a documented initiation phenomenon
In published pharmacology research, the most characteristic early observation is the agonist flare. Reviews of LHRH-analogue action document that the first days of continuous superagonist exposure transiently elevate luteinizing hormone, follicle-stimulating hormone, and downstream sex steroids before suppression sets in.[12] In the three-month sustained-release prostate-adenocarcinoma study, this surge appeared as an early plasma spike preceding the descent of testosterone into the castrate range by roughly day 22.[13] Because the flare is an on-target consequence of the superagonist mechanism rather than an off-target toxicity, it is the single most important confound to anticipate when interpreting early-timepoint data in any HPG-axis model.
Hypogonadal adverse-event profile documented in trials
In published clinical research, the dominant tolerability signal is the expected consequence of profound sex-steroid suppression. The early human pharmacology co-authored by Schally’s group documented that daily D-Trp₆-LHRH drove plasma testosterone and dihydrotestosterone to castrate values, with the effect reversing after discontinuation — establishing both the hypogonadal state and its reversibility as research findings.[14] Reviews of six-month GnRH-agonist depots report that triptorelin pamoate sustains serum testosterone at or below 50 ng/dL — the chemical-castration threshold — in the large majority of subjects across pivotal trials, the documented basis for the hypogonadal adverse-event class associated with the molecule in androgen-suppression research.[15] In reproductive research, by contrast, depot triptorelin used for pituitary down-regulation was reported to achieve effective suppression without a premature LH surge, illustrating that the observed tolerability signature is dose-, schedule-, and context-dependent rather than fixed.[16]
For experimental design, the practical implication is that the flare and the suppression phase are distinct windows with distinct readouts; conflating them obscures the underlying pharmacology. Researchers handling the lyophilized reagent should follow general peptide-integrity practices in the peptide storage guide, and the regulatory boundary between this research reagent and the approved formulations is detailed in research-grade vs pharmaceutical-grade peptides.
Sourcing Research-Grade Triptorelin
For HPG-axis research that depends on a faithfully characterized GnRH superagonist, sourcing comes down to verifiable identity and purity. Apex supplies triptorelin acetate as a lyophilized chemical reagent specified at ≥99% purity, with identity confirmed by HPLC and electrospray-ionization mass spectrometry (ESI-MS) and a lot-specific certificate of analysis archived in the lab-verified COA archive. The verification methodology is documented in the editorial standards, and broader category context lives in the specialty research peptides hub and the wider research library.
Triptorelin is most informative when studied alongside the rest of the GnRH circuit — native GnRH as the pulsatile comparator and the upstream regulators that drive its release. The reagents below support that comparative work; all are supplied for in-vitro and preclinical research only, not for human consumption.
triptorelin and Adjacent Research Reagents
Triptorelin Acetate
GnRH superagonist decapeptide (D-Trp6 substitution) research reagent; supplied at ≥99% purity verified by HPLC and mass spectrometry.
View ProductGonadorelin Acetate
Native GnRH decapeptide; the unmodified comparator for HPG-axis research.
View ProductKisspeptin-10
Upstream KISS1R agonist regulating GnRH release; HPG-axis research reagent.
View ProductBefore placing any reagent into an experiment, confirm the lot-specific COA and handling requirements; the molecule’s integrity is the foundation on which reproducible HPG-axis data is built.
Frequently Asked Questions
What is triptorelin and how does it work?
Triptorelin is a synthetic decapeptide gonadotropin-releasing hormone (GnRH/LHRH) receptor superagonist, structurally native GnRH with a D-tryptophan substituted for glycine at position 6 (D-Trp6-LHRH). In research models, continuous receptor occupancy first produces a brief agonist flare, then drives pituitary GnRH-receptor desensitization and downregulation, ultimately suppressing luteinizing hormone, follicle-stimulating hormone, and downstream sex-steroid output. It is studied as a tool for interrogating the hypothalamic-pituitary-gonadal axis.
Why does a GnRH agonist suppress hormones if it is an agonist?
It is a paradox of receptor pharmacology. Native GnRH is released in pulses; continuous, non-pulsatile stimulation by a long-acting superagonist such as triptorelin desensitizes and downregulates the pituitary GnRH receptor. Published mechanistic work describes agonist-induced receptor phosphorylation, beta-arrestin association, and internalization, alongside altered gonadotropin-subunit biosynthesis. After an initial flare, the net effect reported in the literature is profound suppression of LH, FSH, and sex steroids.
What is the half-life of triptorelin, and how do depot forms change it?
Reported pharmacokinetics show route dependence: subcutaneous administration gives an effective half-life roughly an order of magnitude longer than intravenous dosing, because the peptide releases progressively from the injection-site depot rather than clearing as a single bolus. The D-Trp6 substitution itself extends the half-disappearance time several-fold over native GnRH. Engineered microsphere and polymer-matrix depots described in the literature deliberately extend exposure to approximately one, three, or six months from a single administration.
How is research-grade triptorelin reconstituted and stored?
As research handling context, the lyophilized acetate powder is typically reconstituted with a sterile diluent appropriate to the experimental design, then stored as frozen aliquots with freeze-thaw cycles minimized to preserve peptide integrity. Lyophilized material is kept desiccated at minus 20 degrees Celsius, protected from light and moisture. These are general peptide-research practices, not compound-specific stability data; confirm specifics against the lot certificate of analysis. See our reconstitution and storage guides for detailed handling.
What does triptorelin research cover?
Published literature uses triptorelin to study the hypothalamic-pituitary-gonadal axis: GnRH-receptor superagonist mechanism, the flare-then-desensitization sequence, differential LH-beta versus alpha-subunit regulation, and depot pharmacokinetics. Research-context applications in the literature include androgen-suppression and prostate-cancer models, central precocious puberty studies, reproductive and ovarian-stimulation pituitary down-regulation, and in-vitro gonadotroph cell-line models. All such work is investigational; nothing here implies therapeutic use.
What adverse effects has triptorelin shown in published research?
In published research, the documented profile follows from the superagonist mechanism. An initial agonist flare transiently raises LH, FSH, and sex steroids before suppression sets in. The dominant subsequent signal in clinical studies is the hypogonadal state of profound sex-steroid suppression, with testosterone driven into the castrate range and reported reversal after discontinuation. These are research findings framed for context, not patient guidance or claims of safety or efficacy.
How does triptorelin differ from gonadorelin and from GnRH antagonists?
Gonadorelin is native, unmodified GnRH that activates the receptor in physiologic pulses to sustain gonadotropin release; triptorelin is a long-acting superagonist whose continuous occupancy first flares then suppresses the axis. A GnRH antagonist differs again: it blocks the receptor competitively without activating it, producing prompt suppression with no flare. Researchers choose among them based on whether pulsatile stimulation, desensitization, or flare-free blockade fits the experimental question.
Who first developed triptorelin?
Published reviews credit the LHRH-analog program led by Andrew V. Schally, who characterized LHRH and, in the early 1970s, synthesized D-Trp6-LHRH by substituting D-tryptophan at position 6. Early human pharmacology co-authored by Schally’s group demonstrated that the analog drove testosterone to castrate levels reversibly. The molecule was subsequently developed into depot pharmaceutical formulations marketed internationally; attribution to the originating research program is preserved in the literature.
Continue Your Research
Researchers building broader context across the Apex Research Library may find the following references useful:
- Gonadorelin vs Triptorelin: GnRH Guide — Direct comparison of native pulsatile GnRH (gonadorelin) against the continuous-occupancy superagonist triptorelin.
- Kisspeptin-10 Research Guide — The upstream KISS1R agonist that regulates GnRH release; the layer of the HPG axis above triptorelin.
- Specialty Research Peptides — The category hub situating triptorelin among other specialty-cluster research reagents.
- Research-Grade vs Pharmaceutical-Grade Peptides — Why the same molecule in Trelstar and a research reagent occupy categorically distinct regulatory frameworks.
- How to Read a Peptide COA — Interpreting the identity and purity fields that verify a triptorelin lot before use.
- HPLC Testing for Peptide Purity — How reversed-phase HPLC quantifies the >=99% purity specification.
- Peptide Storage Guide — Storage and freeze-thaw practices that preserve lyophilized decapeptide integrity.
Research Use Disclaimer
Research Use Disclaimer. Triptorelin supplied by Apex Laboratory is a research-grade chemical reagent intended exclusively for in-vitro and preclinical research conducted by qualified professionals. It is not a drug, not a dietary supplement, and not for human or veterinary consumption, diagnosis, treatment, or any therapeutic use. Although triptorelin is also the active molecule in the FDA-approved pharmaceutical formulations Trelstar and Triptodur, those products and a research-grade reagent occupy categorically distinct regulatory frameworks — the research-grade material is not a pharmaceutical and is not a therapeutic equivalent to any approved product. All pharmacological observations cited here are summarized from the published literature for research context and do not constitute claims of safety or efficacy. See research-grade vs pharmaceutical-grade peptides for details.
