
Semaglutide is a 31-residue acylated GLP-1 receptor agonist studied for its effects on glucose regulation, body composition, and cardiovascular outcomes. Its long-chain fatty-acid albumin-binding tether extends plasma half-life to roughly seven days, enabling once-weekly dosing in research and clinical contexts. Trial evidence comes from the SUSTAIN, STEP, PIONEER, and SELECT programs — one of the largest randomized evidence bases in modern peptide research.
Semaglutide is the most-studied glucagon-like peptide-1 (GLP-1) receptor agonist in modern endocrine pharmacology. Designed and developed by Novo Nordisk through a structure-activity-relationship program that built on the earlier liraglutide molecule, Semaglutide is a 31-residue acylated GLP-1 analog whose central design innovation is a long-chain fatty-acid albumin-binding tether that extends its plasma half-life to roughly seven days — enabling once-weekly subcutaneous dosing in research and clinical contexts. Across the SUSTAIN, STEP, PIONEER, and SELECT trial programs, Semaglutide has accumulated one of the largest randomized peer-reviewed evidence bases in modern peptide therapeutics. This guide reads Semaglutide as the research literature reads it: a selective GLP-1 receptor agonist whose receptor pharmacology, structural design, and pharmacokinetic profile are the organizing logic.
This guide provides comprehensive coverage of Semaglutide for researchers — covering molecular identity and the Novo Nordisk lineage from Liraglutide, GLP-1 receptor pharmacology and downstream Gαs / cAMP signaling, pharmacokinetics, the SUSTAIN type-2-diabetes trial program, the STEP obesity trial program, the SELECT cardiovascular outcomes trial in obesity without diabetes, the PIONEER oral-formulation program, the Ozempic / Wegovy / Rybelsus regulatory landscape, and the research-grade catalog distinction. For head-to-head comparison with the dual GIP/GLP-1 receptor agonist Tirzepatide, see the dedicated Semaglutide vs Tirzepatide research comparison; this pillar covers Semaglutide as a foundational compound.
Semaglutide at a Glance
- Semaglutide is a 31-amino-acid acylated GLP-1 analog (CAS 910463-68-2; MW 4113.58 g/mol) developed by Novo Nordisk through structure-activity refinement of the earlier Liraglutide molecule
- The molecule is a selective glucagon-like peptide-1 receptor (GLP-1R) agonist with two structural modifications — an Aib substitution at position 8 conferring DPP-4 resistance, and a C18 fatty diacid linker conferring albumin binding and ~165-hour plasma half-life
- Across the SUSTAIN program (Type 2 diabetes) and STEP program (obesity), Semaglutide demonstrated significant glycemic and weight-management efficacy in randomized phase 3 trials, with cardiovascular outcomes confirmed in SUSTAIN-6 (T2D) and SELECT (obesity without diabetes)
- Three FDA-approved pharmaceutical formulations exist for the same molecule: Ozempic (subcutaneous, T2D, FDA-approved December 2017), Wegovy (subcutaneous, chronic weight management, FDA-approved June 2021), and Rybelsus (oral tablet, T2D, FDA-approved September 2019)
- Apex Laboratory’s Semaglutide is a research-grade chemical reagent verified to ≥99% purity by HPLC and mass spectrometry — categorically distinct from the Ozempic / Wegovy / Rybelsus pharmaceutical formulations per the established research-grade-vs-pharmaceutical-grade framework
- Once-weekly subcutaneous dosing is the canonical research-protocol parameter that distinguishes Semaglutide from earlier GLP-1 analogs (Liraglutide once-daily, Exenatide twice-daily); this is a direct consequence of the albumin-binding fatty-acid linker design
What Semaglutide Actually Is — Molecular Identity
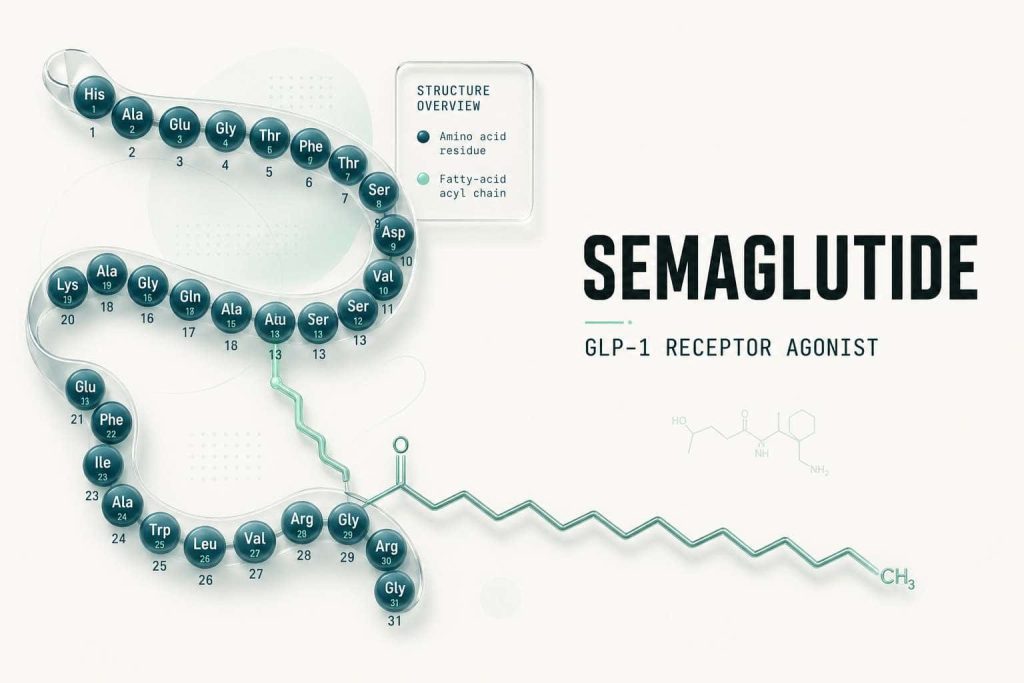
Semaglutide is a synthetic 31-amino-acid peptide that is a structural analog of the endogenous incretin hormone glucagon-like peptide-1 (GLP-1). Its canonical research-literature designation lists CAS registry number 910463-68-2, an empirical molecular formula of C₁₄₄H₂₃₈N₄₂O₆₈, and a molecular weight of 4113.58 g/mol. The peptide retains the canonical GLP-1(7-37) sequence backbone with two distinct chemical modifications that together define its pharmacology and distinguish it from the parent molecule. Knudsen and Lau’s 2019 Frontiers in Endocrinology review “The Discovery and Development of Liraglutide and Semaglutide” remains the most direct historical-attribution reference for the structural lineage from native GLP-1 through Liraglutide and onward to Semaglutide.1
The first modification is an α-aminoisobutyric acid (Aib) substitution at position 8 of the GLP-1 backbone, replacing the native alanine. This single-residue change was specifically engineered to confer resistance to dipeptidyl peptidase-4 (DPP-4), the protease that rapidly cleaves and inactivates native GLP-1 in plasma; the Aib substitution dramatically extends plasma stability without altering receptor-binding affinity. The second and pharmacokinetically larger modification is a C18 fatty diacid (octadecanedioic acid) attached to the lysine at position 26 via a glutamic acid spacer with two short polyethylene glycol-like (8-amino-3,6-dioxaoctanoic acid) linkers. This fatty-acid tether binds reversibly to circulating human serum albumin, dramatically slowing renal and hepatic clearance and extending the plasma half-life to approximately 165 hours (~7 days) — the basis for once-weekly subcutaneous dosing. Lau, Bloch, Schäffer, and colleagues at Novo Nordisk published the canonical structure-activity description of Semaglutide in Journal of Medicinal Chemistry in 2015 — the paper that documented the structural design rationale, receptor binding affinity, and preclinical pharmacokinetic profile that ultimately led to the SUSTAIN and STEP regulatory programs.2
Semaglutide Technical Specifications
- Full Name: Semaglutide
- Trade Names (pharmaceutical): Ozempic, Wegovy, Rybelsus (Novo Nordisk)
- CAS Registry Number: 910463-68-2
- Molecular Weight: 4113.58 g/mol
- Amino Acid Count: 31 residues (GLP-1(7-37) backbone with Aib⁸ substitution)
- Structural Modifications: Aib at position 8 (DPP-4 resistance); C18 fatty diacid linker at Lys26 (albumin binding)
- Plasma Half-Life: ~165 hours (~7 days), supporting once-weekly subcutaneous dosing
- Receptor Target: GLP-1 receptor (GLP-1R), a Class B G-protein coupled receptor coupled to Gαs
- Physical Appearance: White to off-white lyophilized powder
- Solubility: Freely soluble in bacteriostatic water at neutral pH
The Novo Nordisk GLP-1 Program — Lineage from Liraglutide
Semaglutide does not stand alone. It descends from a multi-decade discovery and development program at Novo Nordisk that traces its molecular ancestry back to the original isolation and characterization of glucagon-like peptide-1 in the mid-1980s. Mojsov, Heinrich, Wilson, and colleagues’ 1986 Journal of Biological Chemistry paper “Preproglucagon gene expression in pancreas and intestine diversifies at the level of post-translational processing” was the foundational publication identifying the GLP-1 sequence as a tissue-specific cleavage product of preproglucagon — the discovery that opened the entire incretin pharmacology field that Liraglutide and Semaglutide would later build on.3 Holst’s 2007 Physiological Reviews single-author synthesis “The physiology of glucagon-like peptide 1” is the canonical reference for GLP-1 biology at the time the Novo Nordisk program was advancing the second-generation analog.4
The Novo Nordisk program advanced a sequence of acylated GLP-1 analogs designed to address the central pharmacokinetic limitation of native GLP-1 — a plasma half-life of only one to two minutes due to DPP-4 cleavage and rapid renal clearance. Liraglutide, the first commercial product of this program (FDA-approved 2010 for Type 2 diabetes; later Saxenda for obesity), used a C16 fatty-acid acyl modification with a glutamic acid spacer at Lys26 to confer albumin binding and extend the half-life to approximately 13 hours, supporting once-daily dosing. Semaglutide is the next-generation refinement of the same design strategy: longer C18 fatty diacid (octadecanedioic acid rather than C16 palmitic acid), the Aib⁸ substitution adding DPP-4 resistance, and additional hydrophilic spacer chemistry. Together these changes extend the plasma half-life by an order of magnitude (~13 hours to ~165 hours), enabling the clinically and protocolically distinctive once-weekly dosing schedule.2
The lineage attribution matters editorially. Semaglutide is not a free-standing invention; it is the second-generation Novo Nordisk acylated GLP-1 analog, with Liraglutide as the predecessor compound and shared structural design principles. This contrasts with the parallel Eli Lilly program that produced Tirzepatide (a structurally distinct dual GIP/GLP-1 receptor agonist) and the Eli Lilly Retatrutide molecule (a triple GIP/GLP-1/glucagon receptor agonist) — same therapeutic area, different molecular design lineage. For the head-to-head pharmacology comparison between Semaglutide and Tirzepatide, see the dedicated Semaglutide vs Tirzepatide research guide.
GLP-1 Receptor Pharmacology — Mechanism of Action
The GLP-1 receptor (GLP-1R) is a 463-amino-acid Class B (secretin family) G-protein coupled receptor coupled primarily to Gαs and the adenylate cyclase / cAMP signaling cascade. Drucker’s 2018 Cell Metabolism review “Mechanisms of Action and Therapeutic Application of Glucagon-like Peptide-1” provides the canonical synthesis of GLP-1R signaling, tissue distribution, and downstream effects relevant to the Semaglutide pharmacology literature.5
Receptor Distribution
GLP-1R is expressed across multiple tissue compartments that together explain Semaglutide’s pleiotropic pharmacology. Pancreatic β-cell expression underwrites glucose-dependent insulin secretion. Pancreatic α-cell expression underwrites glucagon suppression at hyperglycemic glucose levels. Gastric and intestinal smooth-muscle expression underwrites the slowed gastric emptying that contributes to postprandial glycemic control. Central nervous system expression — particularly in the arcuate nucleus of the hypothalamus and the area postrema of the brainstem — underwrites the appetite-suppression and satiety effects that are the proximate mechanism of weight loss in the STEP and SELECT trial programs. Cardiovascular GLP-1R expression on cardiomyocytes and vascular endothelium underwrites the cardiovascular outcomes observed in SUSTAIN-6 and SELECT.
Gαs / cAMP Signaling
Semaglutide binding to GLP-1R activates the Gαs subunit, which stimulates adenylate cyclase and elevates intracellular cAMP. In pancreatic β-cells, the elevated cAMP activates protein kinase A (PKA) and the cAMP-responsive guanine nucleotide exchange factor Epac2, both of which potentiate glucose-dependent insulin secretion through actions on the K₊ₘₕ ATP-sensitive potassium channel and on insulin granule trafficking. The glucose-dependence is the pharmacologically important feature: at euglycemic or hypoglycemic glucose levels, the insulin-secretion-potentiation effect is minimal, which is why GLP-1 receptor agonists carry markedly lower hypoglycemia risk than sulfonylureas or insulin in research and clinical contexts.
Insulin Secretion and Glucagon Suppression
The dual effects on the pancreatic islet — enhanced glucose-dependent insulin secretion from β-cells and suppression of inappropriate glucagon secretion from α-cells — together produce the glycemic-control effect that anchors the Type 2 diabetes indication for Ozempic and Rybelsus. Semaglutide does not increase basal insulin secretion (the glucose-dependence preserves physiological feedback control); rather it amplifies the insulin response to elevated glucose while attenuating the glucagon response.
Slowed Gastric Emptying
GLP-1R activation in gastric smooth muscle delays gastric emptying through both vagally-mediated and direct receptor effects. Slowed gastric emptying contributes to postprandial glucose attenuation by reducing the rate at which ingested carbohydrate enters the small intestine for absorption. The same mechanism contributes to satiety signaling and is one of the proximate mechanisms of the gastrointestinal adverse-effect profile (nausea, dyspepsia) commonly reported in clinical trials and research subjects.
Central Appetite and Satiety Signaling
GLP-1R expression in the hypothalamic arcuate nucleus and brainstem area postrema couples to neural circuits that regulate food intake and energy balance. Pro-opiomelanocortin (POMC) neurons in the arcuate are positively modulated by GLP-1R activation, and the brainstem nucleus tractus solitarius receives GLP-1R signaling that influences meal-termination signals. The integrated effect is reduced food intake and increased satiety — the central mechanism that drove the magnitude of weight loss observed in the STEP trial program at the higher 2.4 mg weekly dose. This central pharmacology is also the basis for the chronic weight management indication for Wegovy.
Pharmacokinetics — Albumin Binding and Once-Weekly Dosing
Semaglutide’s pharmacokinetic profile is the engineering achievement that distinguishes it from earlier GLP-1 analogs. The plasma half-life of approximately 165 hours (~7 days) is roughly 100-fold longer than native GLP-1 (~2 minutes) and roughly 13-fold longer than Liraglutide (~13 hours). This extension is achieved through three mechanisms acting in concert: DPP-4 resistance via the Aib⁸ substitution; reversible albumin binding via the C18 fatty diacid tether; and reduced renal clearance secondary to the albumin-bound fraction’s exclusion from glomerular filtration. Steady-state plasma concentrations are typically reached after 4-5 weeks of once-weekly subcutaneous dosing.2
Subcutaneous bioavailability is approximately 89% in human pharmacokinetic studies, with peak plasma concentration (Tmax) reached at approximately 1-3 days post-dose. The volume of distribution is approximately 12.5 L, consistent with predominantly extracellular distribution and substantial albumin binding. Metabolism proceeds via proteolytic cleavage at the peptide backbone and beta-oxidation of the fatty-acid side chain; renal and fecal excretion handle the metabolites. Approximately 3% of an administered dose is excreted unchanged in urine. The combination of long half-life and relatively narrow therapeutic concentration range supports once-weekly dosing while maintaining steady-state plasma exposures.
The oral formulation (Rybelsus) achieves systemic absorption through coformulation with the absorption enhancer salcaprozate sodium (SNAC), which transiently increases gastric epithelial permeability and protects the peptide from local proteolytic degradation in the stomach. Oral bioavailability is approximately 0.4-1% — far lower than the subcutaneous route — necessitating once-daily dosing at a higher milligram dose to achieve comparable steady-state plasma exposure. Aroda and colleagues’ 2019 Diabetes Care publication of the PIONEER-1 randomized clinical trial documented the efficacy of oral Semaglutide monotherapy versus placebo and is the canonical reference for oral-formulation pharmacokinetics in the research literature.6
Receptor Selectivity Across the Incretin Family
Semaglutide is a selective GLP-1 receptor agonist with minimal direct activity at related incretin receptors. This selectivity profile distinguishes it from the dual and triple receptor agonists that have entered the modern incretin pharmacology research literature.
Incretin Receptor Selectivity Across GLP-1 Family Compounds
| Compound | Primary Receptor | Selectivity Profile | Apex Catalog Status |
|---|---|---|---|
| Semaglutide | GLP-1R | GLP-1R selective; minimal GIPR/glucagon-R activity | Apex Semaglutide research-grade ≥99% (Ozempic FDA Dec 2017, Wegovy FDA Jun 2021, Rybelsus FDA Sep 2019 — pharmaceutical formulations categorically distinct) |
| Liraglutide | GLP-1R | GLP-1R selective (predecessor analog) | Apex Liraglutide research-grade ≥99% (Victoza FDA 2010, Saxenda FDA 2014 — pharmaceutical formulations) |
| Tirzepatide | GIPR + GLP-1R (dual) | Dual agonist; GIPR and GLP-1R co-activation | Apex Tirzepatide research-grade ≥99% (Mounjaro FDA 2022, Zepbound FDA 2023 — pharmaceutical formulations) |
| Retatrutide | GIPR + GLP-1R + glucagon-R (triple) | Triple agonist (Eli Lilly investigational; not FDA-approved as of 2026) | Apex Retatrutide research-grade ≥99% (research-only globally) |
| Native GLP-1(7-37) (endogenous reference) | GLP-1R | Endogenous incretin; t½ ~2 min | Endogenous reference; not a catalog SKU |
For deeper context on the dual GIP/GLP-1 mechanism, see the Apex Tirzepatide research guide; for the triple agonist Retatrutide, see the Retatrutide research guide. The cluster-level pillar on the broader incretin family is the GLP-1 / Metabolic research peptides pillar.
SUSTAIN Trial Program — Type 2 Diabetes Evidence
The SUSTAIN clinical-research program comprises a series of phase 3 randomized controlled trials of subcutaneous Semaglutide in adults with Type 2 diabetes. The trials together established the glycemic, weight-loss, and cardiovascular profile that supported the December 2017 FDA approval of Ozempic.
SUSTAIN-1 — Monotherapy vs Placebo
Sorli, Harashima, Tsoukas, and colleagues’ 2017 Lancet Diabetes & Endocrinology publication of SUSTAIN-1 was the first phase 3 randomized trial of once-weekly subcutaneous Semaglutide as monotherapy versus placebo in adults with Type 2 diabetes inadequately controlled with diet and exercise. The trial enrolled 388 participants randomized to Semaglutide 0.5 mg weekly, Semaglutide 1.0 mg weekly, or placebo over 30 weeks; both Semaglutide doses produced significant reductions in HbA1c and body weight versus placebo, establishing the dose-response relationship that the subsequent SUSTAIN program built on.7
SUSTAIN-2 — vs Sitagliptin Add-On
Ahrén, Comas, Jódar, and colleagues’ 2017 Lancet Diabetes & Endocrinology SUSTAIN-2 publication compared once-weekly Semaglutide against once-daily sitagliptin (a DPP-4 inhibitor) as add-on therapy to metformin or thiazolidinediones in 1231 participants over 56 weeks. Semaglutide produced significantly greater reductions in HbA1c and body weight versus sitagliptin, establishing superiority over the DPP-4 inhibitor class as add-on therapy.8
SUSTAIN-3 — vs Exenatide Extended-Release
Ahmann, Capehorn, Charpentier, and colleagues’ 2018 Diabetes Care SUSTAIN-3 publication compared once-weekly Semaglutide against once-weekly exenatide extended-release (the earlier-generation GLP-1 receptor agonist) as add-on therapy in 813 participants over 56 weeks. Semaglutide demonstrated superior glycemic control and weight reduction versus exenatide ER — the first head-to-head comparison establishing Semaglutide’s pharmacodynamic advantage within the GLP-1 receptor agonist class.9
SUSTAIN-7 — vs Dulaglutide
Pratley, Aroda, Lingvay, and colleagues’ 2018 Lancet Diabetes & Endocrinology SUSTAIN-7 publication compared once-weekly Semaglutide (0.5 mg and 1.0 mg) against once-weekly dulaglutide (0.75 mg and 1.5 mg) in 1201 participants over 40 weeks — the head-to-head comparison between Semaglutide and Eli Lilly’s competing once-weekly GLP-1 receptor agonist. Semaglutide demonstrated significantly greater reductions in HbA1c and body weight at both dose-pair comparisons, establishing the within-class efficacy hierarchy that has shaped subsequent meta-analyses.10
SUSTAIN-6 — Cardiovascular Outcomes in Type 2 Diabetes
Marso, Bain, Consoli, and colleagues’ 2016 New England Journal of Medicine publication of the SUSTAIN-6 cardiovascular outcomes trial established the cardiovascular safety and benefit profile of Semaglutide in 3297 participants with Type 2 diabetes and high cardiovascular risk over a median 2.1 years of follow-up. The primary composite endpoint of cardiovascular death, nonfatal myocardial infarction, or nonfatal stroke occurred in significantly fewer participants randomized to Semaglutide versus placebo, with the effect driven primarily by reduction in nonfatal stroke. SUSTAIN-6 was the registrational cardiovascular outcomes trial supporting the Ozempic FDA approval and remains a top-tier reference for the cardiovascular pharmacology of GLP-1 receptor agonists.11
STEP Trial Program — Obesity and Chronic Weight Management
The STEP (Semaglutide Treatment Effect in People with Obesity) clinical-research program comprises a series of phase 3 randomized controlled trials of once-weekly subcutaneous Semaglutide at a higher 2.4 mg dose — well above the 1.0 mg ceiling used in SUSTAIN — in adults with overweight or obesity. The trials established the chronic-weight-management profile that supported the June 2021 FDA approval of Wegovy.
STEP-1 — Adults with Overweight or Obesity
Wilding, Batterham, Calanna, and colleagues’ 2021 New England Journal of Medicine publication of STEP-1 was the registrational phase 3 trial of once-weekly Semaglutide 2.4 mg versus placebo in 1961 adults with body mass index ≥30 (or ≥27 with at least one weight-related comorbidity) without diabetes, over 68 weeks. Mean body weight reduction at week 68 was 14.9% in the Semaglutide arm versus 2.4% in the placebo arm — an effect size that established a new benchmark for pharmacological weight management and that ultimately drove the Wegovy regulatory approval.12
STEP-2 — Adults with Overweight or Obesity and Type 2 Diabetes
Davies, Fábregas, Aroda, and colleagues’ 2021 Lancet publication of STEP-2 evaluated Semaglutide 2.4 mg once-weekly in 1210 adults with both overweight/obesity and Type 2 diabetes over 68 weeks. The dual-population trial established that the higher-dose obesity-indication regimen retained efficacy in the substantial population of adults with both conditions, with body weight reduction of approximately 9.6% in the Semaglutide 2.4 mg arm versus 3.4% in placebo.13
STEP-3 — Combination with Intensive Behavioral Therapy
Wadden, Bailey, Billings, and colleagues’ 2021 JAMA publication of STEP-3 evaluated Semaglutide 2.4 mg once-weekly combined with intensive behavioral therapy (low-calorie diet and physical-activity counseling) versus placebo plus the same intensive behavioral therapy in 611 adults with overweight or obesity over 68 weeks. The trial established the additive effect of pharmacological plus behavioral intervention, with the combination producing significantly greater weight reduction than behavioral therapy alone.14
STEP-4 — Weight Loss Maintenance
Rubino, Abrahamsson, Davies, and colleagues’ 2021 JAMA publication of STEP-4 evaluated continued versus discontinued Semaglutide 2.4 mg once-weekly in adults who had achieved ≥5% weight loss during a 20-week run-in period. Continued treatment produced an additional 7.9% weight reduction over 48 weeks; discontinuation produced a 6.9% regain, establishing the chronic-treatment-dependence profile that frames the obesity research literature.15
SELECT — Cardiovascular Outcomes in Obesity Without Diabetes
Lincoff, Brown-Frandsen, Colhoun, and colleagues’ 2023 New England Journal of Medicine publication of the SELECT trial established cardiovascular outcomes for Semaglutide 2.4 mg once-weekly in 17,604 adults with overweight or obesity and pre-existing cardiovascular disease but without diabetes, over a mean follow-up of 39.8 months. The primary composite endpoint of cardiovascular death, nonfatal myocardial infarction, or nonfatal stroke occurred in 6.5% of the Semaglutide group versus 8.0% of the placebo group — a 20% relative risk reduction. SELECT extended the cardiovascular evidence base from the diabetes population (SUSTAIN-6) to the broader obesity-without-diabetes population, supporting the March 2024 FDA label expansion of Wegovy to include cardiovascular risk reduction in adults with established cardiovascular disease and overweight or obesity.16
PIONEER Program — Oral Semaglutide
The PIONEER (Peptide InnOvatioN for Early diabEtes tREatment) clinical-research program evaluated the oral tablet formulation of Semaglutide that ultimately became Rybelsus (FDA-approved September 2019). Aroda, Rosenstock, Terauchi, and colleagues’ 2019 Diabetes Care publication of PIONEER-1 was the foundational randomized clinical trial of oral Semaglutide monotherapy versus placebo in 703 participants with Type 2 diabetes over 26 weeks; oral Semaglutide produced significant reductions in HbA1c versus placebo at 7 mg and 14 mg daily doses, establishing the oral-formulation efficacy that supported the regulatory pathway for Rybelsus.6
Husain, Birkenfeld, Donsmark, and colleagues’ 2019 New England Journal of Medicine publication of PIONEER-6 was the cardiovascular outcomes trial for the oral formulation, evaluating oral Semaglutide 14 mg daily versus placebo in 3183 participants with Type 2 diabetes and high cardiovascular risk over a median 15.9 months of follow-up. The primary composite cardiovascular endpoint was non-inferior with oral Semaglutide versus placebo, establishing the cardiovascular safety profile required for the Rybelsus FDA approval.17
Ozempic / Wegovy / Rybelsus — Regulatory Framing
Three FDA-approved pharmaceutical formulations exist for the same Semaglutide molecule, each with distinct route, dose, and indication. The regulatory landscape applies the same Cerebrolysin / Vyleesi precedent template that the Apex corpus uses for compounds where a research-grade chemical reagent and one-or-more approved pharmaceutical formulations share the same molecule but operate under categorically distinct regulatory frameworks.
Ozempic — subcutaneous Semaglutide formulated for once-weekly self-administration via auto-injector at 0.25 mg (initial), 0.5 mg, 1.0 mg, or 2.0 mg weekly doses. FDA-approved December 5, 2017 by Novo Nordisk under New Drug Application NDA 209637 for the treatment of Type 2 diabetes mellitus as an adjunct to diet and exercise. The SUSTAIN-1 through SUSTAIN-7 trials anchored the registrational efficacy evidence; SUSTAIN-6 anchored the cardiovascular safety evidence.
Wegovy — subcutaneous Semaglutide formulated at higher 2.4 mg once-weekly dose for chronic weight management. FDA-approved June 4, 2021 by Novo Nordisk under New Drug Application NDA 215256 for chronic weight management in adults with obesity (BMI ≥30) or overweight (BMI ≥27) with at least one weight-related comorbidity. The STEP-1 through STEP-5 trials anchored the registrational evidence. The March 2024 FDA label expansion added cardiovascular risk reduction in adults with established cardiovascular disease and overweight or obesity, anchored by the SELECT trial evidence.
Rybelsus — oral Semaglutide tablet formulated with the absorption enhancer salcaprozate sodium (SNAC), at 3 mg, 7 mg, or 14 mg once-daily doses. FDA-approved September 20, 2019 by Novo Nordisk for Type 2 diabetes mellitus as an adjunct to diet and exercise. The PIONEER-1 through PIONEER-10 trials anchored the registrational evidence; PIONEER-6 anchored the cardiovascular safety evidence.
The Cerebrolysin-precedent regulatory framing matters editorially. Ozempic, Wegovy, and Rybelsus are FDA-approved Semaglutide pharmaceutical formulations for specific clinical indications — documented regulatory facts that the research literature describes in regulatory-fact terms. Apex Laboratory’s Semaglutide is a research-grade chemical reagent, lyophilized powder, ≥99% purity by HPLC and mass spectrometry, intended exclusively for in-vitro and preclinical research. Same molecule (Semaglutide); categorically distinct regulatory frameworks. Apex’s research-grade material is not a pharmaceutical product, is not therapeutically equivalent to Ozempic / Wegovy / Rybelsus, and is not framed in this guide as a substitute for or alternative to the FDA-approved pharmaceutical formulations.
The same regulatory-precedent template is used elsewhere in the Apex corpus — see the Cerebrolysin Research Guide for the parallel per-jurisdiction framing template, and the research-grade vs pharmaceutical-grade peptides framework for the categorical distinction across the Apex catalog.
Research-Grade vs Pharmaceutical-Grade — The Apex Catalog Distinction
The framework anchor for the Ozempic/Wegovy/Rybelsus-vs-Apex catalog distinction is the LIVE Lab Methods cluster article on research-grade vs pharmaceutical-grade peptides, which establishes the categorical distinction across the Apex corpus. The framework applies cleanly to Semaglutide:
Pharmaceutical formulations (Ozempic / Wegovy / Rybelsus) — manufactured under Good Manufacturing Practice (GMP) for clinical use; supplied through the prescription pharmaceutical distribution channel; carry FDA-approved indications and labels specifying dosing, contraindications, and adverse-event profile; sponsor Novo Nordisk under NDA 209637 (Ozempic), NDA 215256 (Wegovy), and the Rybelsus NDA.
Apex catalog Semaglutide — research-grade chemical reagent, lyophilized powder, ≥99% purity verified per batch by HPLC and mass spectrometry per the ≥99% purity standard and mass-spectrometry verification protocol documented in the lab-verified COA archive; supplied through the research-reagent vendor channel for in-vitro and preclinical research applications. NOT a pharmaceutical product; NOT for human consumption.
Same molecule (Semaglutide); categorically distinct regulatory frameworks. Researchers building broader vendor and grade-discrimination context may also find the vendor evaluation checklist and the Editorial Standards page useful for the analytical-chain documentation that distinguishes Apex’s research-grade material from less-rigorous reagent suppliers.
Reading Semaglutide Research Papers — What GLP-1R Selectivity Changes
For researchers reading Semaglutide literature for the first time, the single most useful interpretive frame is receptor selectivity. The GLP-1R-selective profile changes what conclusions the literature can support. Studies using Semaglutide are characterizing GLP-1R-selective pharmacology — pancreatic islet effects, central appetite regulation via hypothalamic GLP-1R, gastrointestinal effects via gastric and intestinal GLP-1R, and cardiovascular effects via cardiomyocyte and endothelial GLP-1R. Studies using Tirzepatide (dual GIPR/GLP-1R) characterize incretin pharmacology blending the two receptor contributions. Studies using Retatrutide (triple GIPR/GLP-1R/glucagon-R) add glucagon-receptor pharmacology to the mix.
This receptor-selectivity discipline matters when reading meta-analyses and indirect comparisons in particular. Within-class comparisons (e.g., Semaglutide vs Liraglutide vs Dulaglutide vs Exenatide) hold the receptor target constant and vary the pharmacokinetic profile or specific structural modifications; these comparisons inform pharmacological-class hierarchy questions. Between-class comparisons (Semaglutide vs Tirzepatide) introduce additional receptor pharmacology and require careful attribution of observed differences to GIPR pharmacology versus pure receptor-binding-affinity variation. The Knudsen and Lau 2019 Frontiers in Endocrinology review provides the canonical lineage framing for the within-class hierarchy.1
The companion Apex Semaglutide vs Tirzepatide research comparison provides the head-to-head between-class reading frame. The companion GLP-1 / Metabolic research peptides pillar covers the broader incretin-family research-peptide architecture.
Sourcing Semaglutide for In-Vitro and Preclinical Research
Apex Laboratory supplies Semaglutide as a research-grade chemical reagent at ≥99% purity, verified by HPLC and mass spectrometry on every batch and documented through the lab-verified COA archive per the editorial standards — the Apex Semaglutide catalog product is a lyophilized powder for in-vitro and preclinical research applications, distinct from any pharmaceutical formulation. Procedural references on peptide reconstitution, cold-chain storage, Certificate of Analysis verification, research-context dosing calculation, and HPLC purity verification document the analytical chain.
Researchers building broader incretin-family research context may find the related Apex catalog products useful: Semaglutide (GLP-1R-selective), Liraglutide (GLP-1R-selective predecessor), Tirzepatide (dual GIPR/GLP-1R), and Retatrutide (triple GIPR/GLP-1R/glucagon-R).
Incretin Research Reagents
Semaglutide
31-residue acylated GLP-1 analog research reagent; selective GLP-1R agonist with C18 fatty diacid albumin-binding linker; supplied at ≥99% purity verified by HPLC and mass spectrometry.
View ProductTirzepatide
Dual GIPR/GLP-1R agonist research reagent; 39-residue acylated peptide; structural design distinct from the Novo Nordisk GLP-1 analog lineage.
View ProductRetatrutide
Triple GIPR/GLP-1R/glucagon-R agonist research reagent; investigational compound for incretin-family pharmacology research; not FDA-approved.
View ProductFrequently Asked Questions
What is Semaglutide?
Semaglutide is a synthetic 31-amino-acid acylated analog of glucagon-like peptide-1 (GLP-1), with CAS registry number 910463-68-2 and molecular weight 4113.58 g/mol. It is a selective agonist of the GLP-1 receptor (GLP-1R), developed by Novo Nordisk through structure-activity refinement of the earlier Liraglutide molecule. Apex Laboratory supplies Semaglutide as a research-grade chemical reagent at ≥99% purity for in-vitro and preclinical research, distinct from the Ozempic, Wegovy, and Rybelsus pharmaceutical formulations.
How does Semaglutide work mechanistically?
Semaglutide acts as a selective agonist of the GLP-1 receptor — a Class B G-protein coupled receptor coupled primarily to Gαs and the adenylate cyclase / cAMP signaling cascade. GLP-1R activation in pancreatic β-cells potentiates glucose-dependent insulin secretion; in α-cells suppresses glucagon at hyperglycemic levels; in gastric and intestinal smooth muscle slows gastric emptying; and in hypothalamic and brainstem neurons modulates appetite and satiety signaling. Drucker 2018 in Cell Metabolism is the canonical mechanism reference.
What is the difference between Semaglutide, Ozempic, Wegovy, and Rybelsus?
All four refer to the same Semaglutide molecule. Ozempic is the subcutaneous formulation FDA-approved in December 2017 for Type 2 diabetes (NDA 209637). Wegovy is the higher-dose 2.4 mg subcutaneous formulation FDA-approved in June 2021 for chronic weight management (NDA 215256). Rybelsus is the oral tablet formulation co-formulated with the absorption enhancer SNAC, FDA-approved in September 2019 for Type 2 diabetes. Apex Laboratory’s Semaglutide is a research-grade chemical reagent for in-vitro and preclinical research, categorically distinct from the three pharmaceutical formulations.
Why is Semaglutide dosed once weekly?
The once-weekly dosing schedule is a direct consequence of Semaglutide’s engineered pharmacokinetic profile. Two structural modifications — an Aib substitution at position 8 conferring DPP-4 resistance, and a C18 fatty diacid linker at Lys26 conferring albumin binding — together extend the plasma half-life to approximately 165 hours (~7 days). Steady-state plasma concentrations are reached after 4-5 weeks of once-weekly subcutaneous dosing. Lau et al. 2015 in Journal of Medicinal Chemistry is the canonical structural design reference.
How is Semaglutide different from Liraglutide?
Liraglutide is the predecessor compound from the same Novo Nordisk acylated GLP-1 analog lineage; both molecules use the strategy of fatty-acid acylation to confer reversible albumin binding. Semaglutide differs in three ways: a longer C18 fatty diacid linker (versus C16 palmitic acid in Liraglutide); the Aib substitution at position 8 conferring DPP-4 resistance; and additional hydrophilic spacer chemistry. Together these changes extend the plasma half-life from ~13 hours (Liraglutide, daily dosing) to ~165 hours (Semaglutide, weekly dosing).
How is Semaglutide different from Tirzepatide?
Semaglutide is a selective GLP-1 receptor agonist with minimal activity at related incretin receptors. Tirzepatide is a structurally distinct dual GIPR/GLP-1R agonist developed by Eli Lilly — it activates both the GIP receptor and the GLP-1 receptor. The selectivity difference matters for what conclusions the literature can support: Semaglutide studies characterize GLP-1R-selective pharmacology; Tirzepatide studies characterize incretin pharmacology blending GIPR and GLP-1R contributions. See the dedicated Semaglutide vs Tirzepatide comparison guide for head-to-head pharmacology.
Is Semaglutide approved for human therapeutic use?
Yes — in three FDA-approved pharmaceutical formulations: Ozempic (subcutaneous, T2D, December 2017), Wegovy (subcutaneous, chronic weight management, June 2021; cardiovascular risk reduction added March 2024), and Rybelsus (oral, T2D, September 2019). Apex Laboratory’s Semaglutide is NOT a pharmaceutical product. It is a research-grade chemical reagent intended exclusively for in-vitro laboratory and preclinical research. It is not for human consumption, not therapeutically equivalent to the FDA-approved formulations, and not promoted as a substitute for them.
Continue Your Research
Researchers building broader GLP-1, incretin, and metabolic research-peptide context across the Apex library may find the following references useful:
- GLP-1 / Metabolic Research Peptides Pillar — cluster-level pillar covering the incretin-family architecture (Semaglutide, Liraglutide, Tirzepatide, Retatrutide, AOD9604)
- Semaglutide vs Tirzepatide Research Comparison — head-to-head between-class comparison
- Tirzepatide Research Guide — dual GIPR/GLP-1R agonist sister Tier-1 compound guide
- Retatrutide Research Guide — triple GIPR/GLP-1R/glucagon-R agonist sister Tier-1 compound guide
- Retatrutide vs Tirzepatide Research Comparison — lateral within-cluster comparison
- Research-Grade vs Pharmaceutical-Grade Peptides — Lab Methods cluster framework anchor for the Ozempic/Wegovy/Rybelsus-vs-Apex distinction
- Vendor Evaluation Checklist — Lab Methods vendor-discrimination reference
- ≥99% Purity Standard and Mass Spectrometry Verification — analytical-chain documentation
- Procedural references: reconstitution, storage, dosing calculation, COA verification, HPLC purity verification
Research Use Disclaimer
This article is provided for educational and research reference purposes only. Semaglutide and all products sold by Apex Laboratory are intended exclusively for in-vitro laboratory and preclinical research use and are not for human consumption. Apex Laboratory’s research-grade Semaglutide is a chemical research reagent distinct from the Ozempic, Wegovy, and Rybelsus pharmaceutical formulations (FDA-approved by Novo Nordisk for Type 2 diabetes and chronic weight management indications); this article describes the research-reagent context only and does not endorse, describe procedures for, or imply therapeutic equivalence between the research-grade chemical reagent and the FDA-approved pharmaceutical formulations. Documented findings in animal models, cellular research assays, and randomized clinical trials in human populations should not be extrapolated to human-clinical claims for the research-grade catalog product. Researchers should consult the primary peer-reviewed literature cited throughout this article for detailed methodological protocols, experimental designs, and complete data sets.
